Last Updated on October 28, 2023
The term cold abscess refers to an abscess [An Abscess is a collection of liquefied tissue(pus) in the body] where typical signs of abscess [warmth, redness, tenderness,] are absent. The prefix cold indicates that the abscess is not hot because that is the usual case.
Thus a cold abscess is not accompanied by the classical signs of inflammation- heat, redness, fever, pain etc., which are usually found with the pyogenic abscess.
The only conditions when a cold abscess shows sign of inflammation are
- When it is about to burst out of the skin
- When there is a mixed infection with pyogenic organisms.
A cold abscess is typically seen in tubercular infection but can be encountered in actinomycosis, blastomycosis, and leprosy.
Cold abscesses are most commonly associated with osteoarticular tuberculosis and lymph node tuberculosis.
Pathogenesis of Cold Abscess Formation
The characteristic microscopic lesion in tuberculosis is the tuberculous granuloma– a collection of epithelioid and multinucleated giant cells in the periphery. Within the tubercle, small patches of caseous necrosis appear. These may coalesce into a larger yellowish mass and the center may break down to form an Abscess.
Thus cold abscess is formed by a collection of products of liquefaction & the reactive exudates.
After formation of the abscess, continuous disease activity may build up the pressure further and the cold abscess breaks its boundaries, penetrates the ligaments in articular disease, bone & periosteum in osseous disease.
Further buildup makes the cold abscess to migrate in various directions following the path of least resistance along fascial planes, blood vessels and nerves to appear superficially at distant sites away from the site of the lesion.
In the lymph nodes, periadenitis results in matting and fixity of lymph nodes. The lymph nodes coalesce and breakdown to form caseous pus which may perforate the deep fascia and present as fluctuant swelling on the surface.
The overlying skin becomes indurated, breaks down and leads to the formation of a sinus.
The cold abscess is composed of
- Serum
- Leucocytes
- Caseous material
- Bone debris
- Tubercle bacilli
Sometimes, the cold abscesses may get secondarily infected by pyogenic bacteriae and present as a hot abscess.
Sites of Cold Abscess
Cold abscesses are most commonly seen in
- Neck & Axilla
- Back
- Side of chest wall
Clinical Features
There would be a painless swelling of insidious onset without any history of high fever. The slight rise of temperature is seen in tuberculosis and is due to disease activity.
On examination, there would be a mass of soft and cystic consistency. The swelling would have fluctuations and there would be no transillumination. By large the swelling is not compressible though in some cases where the apparent abscess communicates with an underlying cavity, the size may reduce on the application of pressure.
Often the patient has other features suggestive of tuberculosis. If not, location of the abscess could indicate as a rough guide to the region involved.
Additional sinuses may be present.
Sometimes, the only presentation of tuberculosis is a cold abscess and work up to find underlying lesion may be required.
The abscess would cause local Pressure effects too especially the deep cold abscesses.
For example in the cervical spine, the exudate collects behind prevertebral fascia & protrude forward as retropharyngeal abscess which may cause dysphagia, dysphonia, dyspnoea and/or hoarseness of voice
Laterally, it may spread into the sternomastoid muscle & present as swelling in the neck.
The abscess may trickle down to mediastinum to along trachea or esophagus.
In the thoracic spine, the collection may cause the formation of a paravertebral abscess. It also may enter into spinal canal & cause extradural compression of the cord.
It can penetrate the anterior longitudinal ligament to form a mediastinal abscess or through the medial arcuate ligament to form a lumbar abscess.
IT may appear anywhere along the course of intercoastal nerve too.
In the lumbar spine, the pus can track along the psoas muscle towards the groin & presents as psoas abscess. It might lead to flexion of the hip, a condition termed as pseudo flexion deformity of hip>
It can travel along the iliopsoas tendon to appear on the medial aspect of the thigh.
It can spread laterally beneath iliac fossa to emerge at the iliac crest near the anterior superior iliac spine. The pus can also form an abscess in Scarpa’s triangle or gluteal region.
Differential diagnosis
- Lipoma
- Cyst
- Soft tissue tumors
Diagnostic Work Up
Most of the cold abscesses are evident from their history, location and examination findings. The workup should include finding the tubercular lesion.
Routine blood works will show increased lymphocytes, raised ESR and CRP.
Antigravity aspiration and study for tuberculous bacteria are initiated which include PCR and culture of the aspirate. Stain for acid-fast bacilli is not positive often due to paucibacillary nature of osteoarticular tuberculosis.
X-ray and MRI are useful imaging studies. CT is able to assess bone destruction better.
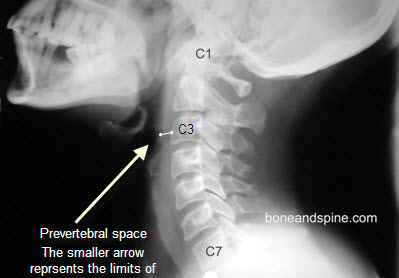
In the cervical region, retropharyngeal abscess may be seen on lateral x-ray [Soft tissue shadow thickness in front of C3 vertebra >4mm].
Normal limits are shown in x-ray.
Paravertebral shadow on AP view indicates paravertebral abscess in the thoracic spine. Psoas shadow may be obliterated on x-ray in case of psoas abscess.
MRI gives a better assessment of extradural abscesses / subligamentous spread. It can also reveal skip lesions and spinal cord compression.
Treatment of Cold Abscess
The cold abscess is not the primary culprit. Underlying tuberculosis is. Therefore the treatment is for underlying tuberculosis. As underlying tuberculosis heals, the cold abscess would reduce at first and then go away.
The treatment of tuberculosis is by use of antitubercular drugs.
[Read more on the treatment of tuberculosis]
Some cold abscesses are large and would need a reduction of the fluid load for drugs to reach the site.
The aspiration is done in an antigravity fashion in a zig-zag method, so as to avoid fistula formation from continuous gravitational drainage through the puncture site.
For very large cold abscess, ultrasound-guided Pigtail catheter drainage or open surgical drainage is considered.