Last Updated on March 13, 2020
The humerus is a bone that connects the shoulder and elbow. The humerus is the largest bone in the upper limb and the only bone in the upper arm. Humerus movements participate in many days to day essential activities like throwing, lifting, writing and others which require movements of the shoulder joint.
Proximally, humerus forms part of the shoulder joint whereas distally, the humerus articulates with the radius and ulna to form the elbow joint.
The humerus bone acts as an attachment site for many important muscles and ligaments.
Structure of Humerus Bone
For describing the anatomy of the humerus bone, it is divided into three parts
- Proximal end
- Shaft
- Distal end
Proximal End of Humerus
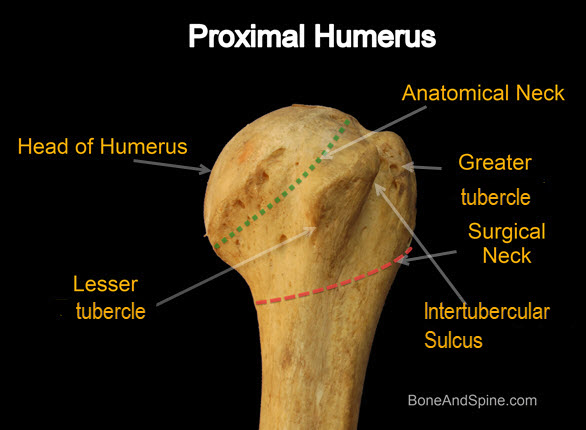
Head is the most proximal region of the bone. The Head is almost spherical in shape and flattens a bit where it attaches to the scapula and clavicle.
The head is directed medially, backward and upwards. It articulates with the glenoid cavity of the scapula to form the shoulder joint. The head forms about one-third of a sphere and is much larger than the glenoid cavity.
The line separating the head from the rest of the upper end is called the anatomical neck.
There are two tubercles present.
The lesser tubercle is an elevation on the anterior aspect of the upper end.
The greater tubercle is an elevation that forms the lateral part of the upper end. Its posterior aspect is marked by three impressions-upper, middle and lower.
Bicipital groove separates the lesser tubercle (medially) from the anterior part of the greater tubercle. The sulcus has medial and lateral lips that represent downward prolongations of the lesser and greater tubercles and serves for the attachment of ligaments and muscles
The line separating the upper end of the humerus from the shaft is called the surgical neck.

Shaft of Humerus
The shaft is rounded in the upper half and triangular in the lower half. It has three borders and three surfaces.
Borders
The anterior border is a continuation of the lateral lip of the intertubercular sulcus or bicipital groove. In its middle part, it forms the anterior margin of the deltoid tuberosity. The lower half of the anterior border is smooth and rounded.
The lateral border is prominent only at the lower end where it forms the lateral supracondylar ridge. In the middle part, it is interrupted by the radial (spiral) groove which holds the radial nerve.
The medial lip of the intertubercular sulcus or bicipital groove continues as the medial border. About its middle, it presents a rough strip. It is continuous below with the medial supracondylar ridge.
Surfaces
Anterolateral surface lies between the anterior and lateral borders. The upper half of this surface is covered by the deltoid. It is marked by a V-shaped deltoid tuberosity a little above the middle.
The anteromedial surface lies between the anterior and medial borders. Its upper one third is narrow and forms the floor of the bicipital groove. Near the medial border, at almost middle, a nutrient foramen is seen.
Between the medial and lateral borders lies the posterior surface. It is marked by an oblique ridge in the upper part and is crossed by the radial groove in the middle third.
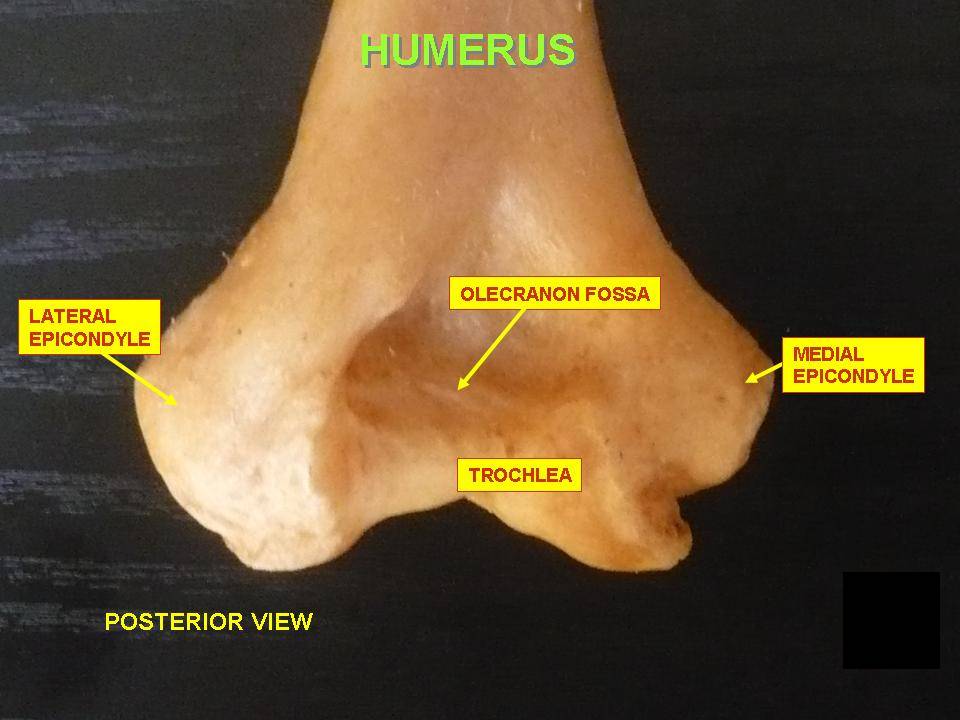
Lower End of Humerus
Below the deltoid tuberosity, the humerus gradually widens, doubling its width as it approaches the elbow.
The lower end of the humerus forms the condyle which is expanded from side to side and shows lateral supracondylar ridge and the medial supracondylar ridge is a similar ridge on the medial side.

Articular part
- The capitellum is a rounded projection that articulates with the head of the radius to form radiocapitellar joint.
- The trochlea is a pulley shaped surface. It articulates with the trochlear notch of the ulna to form the elbow joint. The medial edge of the trochlea projects down 6 mm more than the lateral edge. This leads to a carrying angle or the angle by which forearm projects from the humeral axis.
Nonarticular part
On the medial and lateral side, there are prominent bony projections called epicondyle. Medial is called the medial epicondyle and lateral one is termed as the lateral epicondyle.
The lateral epicondyle is smaller than the medial epicondyle.
The coronoid fossa is a depression just above the anterior aspect of the trochlea. It accommodates the coronoid process of the ulna when the elbow is flexed.
The radial fossa is a depression present just above the anterior aspect of the capitulum. It accommodates the head of the radius when the elbow is flexed.
The olecranon fossa lies just above the posterior aspect of the trochlea. It accommodates the olecranon process of the ulna when the elbow is extended.
Attachments of Humerus
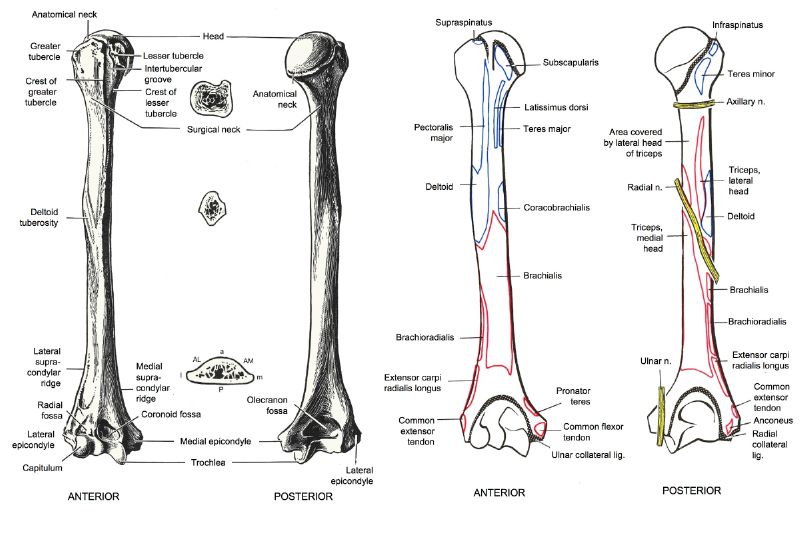
Upper Humerus
The subscapularis is inserted into the lesser tuberosity.
The greater tuberosity gives attachment to insertion of supraspinatus, infraspinatus and teres minor.
- Supraspinatus -uppermost part
- Infraspinatus – Middle
- Teres minor- lower impression
Intertubercular sulcus also gives attachment to the insertion of three muscles. The pectoralis major inserts into the lateral lip of the intertubercular sulcus in two layers. The teres major is inserted into the medial lip of the intertubercular sulcus. The latissimus dorsi is inserted into the floor of the intertubercular sulcus.
[The contents of the intertubercular sulcus are the tendon of the long head of the biceps and its synovial sheath along with the ascending branch of the anterior circumflex humeral artery.]
The anatomical neck provides attachment to the capsular ligament of the shoulder joint except on the medial side. On the medial side, the line of attachment dips down by about a centimeter to include a small area of the shaft within the joint cavity.
An aperture is provided for the tendon of the long head of the biceps leaves the joint cavity
Shaft of Humerus
The deltoid tuberosity provides insertion to the deltoid muscle.
A rough area in the middle of the medial border is for the insertion of coracobrachialis.
The brachialis arises from the lower halves of the anteromedial and anterolateral surfaces of the shaft extending in part on to the posterior aspect.
Lower End
Upper two-thirds of the lateral supracondylar ridge give origin to brachioradialis whereas the lower one third gives rise to extensor carpi radialis longus.
The anteromedial surface, near the lower end of the medial supracondylar ridge, gives origin to the humeral head of pronator teres. {The other end arises from ulna on the medial side of the coronoid}
The common flexor origin on the anterior aspect of the medial epicondyle gives rise to superficial flexors of wrist and hand, commonly called flexor forearm muscles. These are flexor carpi ulnaris, palmaris longus, flexor carpi radialis and pronator teres
The common extensor origin on lateral epicondyle provides origin to the extensor muscles of the forearm. These muscles are brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorium, extensor digiti minimi, and extensor carpi ulnaris.
The posterior surface of the lateral epicondyle gives rise to the anconeus muscle.
The capsular of the elbow joint is attached along a line that reaches proximal to the radial and coronoid fossae, anteriorly, and on the posterior side, proximal to the olecranon fossa posteriorly.
On the medial side, the line of attachment of the capsule passes between the medial epicondyle and the trochlea. On the lateral side, it passes between the lateral epicondyle and the capitellum.
Side Determination of Humerus Bone
- The upper end is rounded to form the head. The lower end is expanded from side to side and flattened from before backward.
- The head is directed medially and backward.
- The lesser tubercle projects from the front of the upper end and is limited laterally by the intertubercular sulcus (bicipital groove)
Ossification of Humerus
The humerus is ossified from eight centers, one for each of the following parts of humerus – the body, the head, the greater tubercle, the lesser tubercle, the capitellum, the trochlea, and one for each epicondyle.
There are one primary and seven secondary centers.

Primary Center
The center for the body appears near the middle of the diaphysis in the eighth week of fetal life and soon extends toward the extremities. This is the primary center.
At birth the humerus is ossified in nearly its whole length, only the extremities remaining cartilaginous.
Upper End of Humerus
The ossification centers appear as follow
- Head of the bone – First year
- Greater tubercle – second year
- Lesser tubercle – Fifth year
Centers for the head and tubercles join by 6 years to form a single large epiphysis. This fuses with the body about the twentieth year.
Lower End of Humerus
The ossification centers for lower end are remembered by CRITOE. That is the order of appearance.

The timeline is as follows
- Capitellum – 1-2 year
- Radius – 3-4year
- Internal or medial epicondyle – 5-6 years
- Trochlea – 8 years
- Olecranon – 9-10 years
- External or lateral epicondyle – 11-12 years
About the sixteenth or seventeenth year, the lateral epicondyle and both portions of the articulating surface, having already joined, unite with the body, and at the eighteenth year, the medial epicondyle becomes joined to it.