Last Updated on October 29, 2023
Ankle fractures are actually groups fractures involving different parts of the region – the distal tibia, distal fibula, talus, and calcaneus. More often they are referred to fractures involving malleoli, distal tibia, and fibula.
But ankle fractures also include the fractures of talus and calcaneum along with above-mentioned injuries. The group also includes fracture pattern including the distal tibia, medial malleolus, lateral malleolus, posterior malleolus, distal fibula, syndesmosis between distal tibia and fibula, talus and calcaneum. Ankle subluxation or dislocation may accompany these fractures. In such cases, the term ‘ankle fracture and dislocation’ is used.
The frequency of ankle fractures has been increasing for the past 20 years and occurs more commonly in males than in females.
Most patients younger than 50 years are male, while most older than 50 years are female.
Anatomy of Ankle Joint and Pathophysiology of Injuries
As noted, ankle fractures refer to fractures of the distal tibia, distal fibula, talus, and calcaneus.
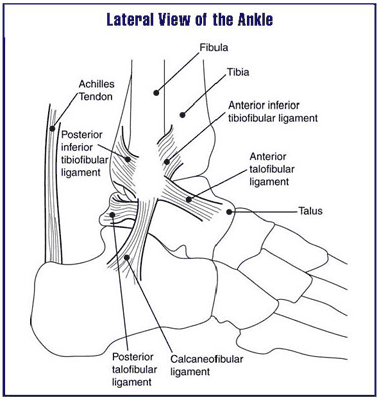
The ankle joint is formed by the distal end of tibia including its projections called medial malleolus and posterior malleolus, the distal part of the fibula known as lateral malleolus, intervening syndesmosis between the fibula and tibia. This structure articulates with the dome of the talus to form an ankle joint or tibiotalar joint.
Talus atops calcaneum and forms subtalar joint or talocalcaneal joint. The primary motion of the ankle at the true ankle joint) is plantarflexion and dorsiflexion. Inversion and eversion occur at the subtalar joint. Because inversion and eversion are integral parts occurring with ankle motions, injuries to calcaneus or subtalar joints affect the ankle motion.
Excessive inversion stress is the most common cause of ankle injuries as the medial malleolus is shorter than the lateral malleolus, allowing the talus to invert more than it everts. Secondly, the lateral support is weaker as compared to medial support offered by deltoid.
Therefore, the ankle is more stable and resistant to eversion injury than inversion injury. But eversion injury, when it occurs, requires a substantial force and infers quite a damage to bony and ligamentous supports.
The ankle joint usually adheres to the ring axiom (eg, a fracture in one part of the ring often is associated with a second injury). For example, a fracture of the medial malleolus may also be associated with either a lateral malleolar fracture or rupture of the lateral ligaments.
Clinical Presentation of Ankle Fractures
A patient presenting with an ankle injury should be evaluated for other possible injuries as well.
There would be swelling and deformity of the ankle, bony tenderness and ecchymosis. In minimal trauma, all other signs other than the tenderness of bone may be absent.
Fracture with external wounds should be deemed open unless ruled out.
Inspect carefully for the presence of open wounds close to the injured ankle.
Assess the neurovascular, the ipsilateral knee and foot
Different Ankle Fractures
Malleolar Fractures
Following injury-patterns are seen
- Isolated medial malleolus fracture
- Isolated lateral malleolus fracture
- Bimalleolar [Pott fracture] – included fracture of both medial and lateral malleolus
- Bimalleolar-equivalent fractures – In addition to one of the malleoli fracture, the ligaments on the other malleolus side are injured.
- Posterior malleolus fractures
- Bosworth fracture-dislocation
- Rare fracture of the distal fibula with
- Associated fixed posterior dislocation of the proximal fibular fragment which becomes trapped behind the posterior tibial tubercle.
- Caused by severe external rotation of the ankle.
- Associated syndesmotic injuries
- Cotton fracture
- A trimalleolar fracture
- Involves the medial, lateral, and posterior malleoli
Pilon fracture
A pilon fracture designates a fracture of the distal tibial metaphysis combined with disruption of the talar dome.

Maisonneuve fracture
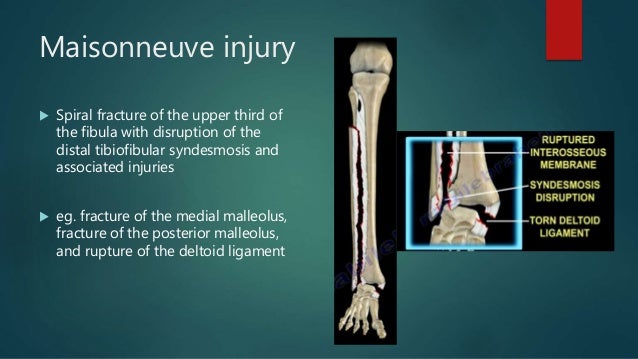
A Maisonneuve fracture, , is a proximal fibular fracture coexisting with a medial malleolar fracture or disruption of the deltoid ligament. Maisonneuve fractures are associated with partial or complete disruption of the syndesmosis.
Tillaux fracture
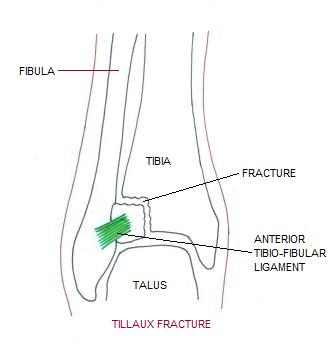
Tillaux fracture is a Salter-Harris (SH) type III injury of the anterolateral tibial epiphysis caused by extreme eversion and lateral rotation of the ankle. Incidence is highest in adolescents, usually those aged 12-14 years, because the fracture occurs after the medial aspect of the epiphyseal plate of the tibia closes but before the lateral aspect arrests.
Snowboarder’s fracture
It is a fracture of the lateral process of the talus, seen commonly in snowboarders, hence the name.
A combination of dorsiflexion and inversion of the ankle produces the lateral talar fracture.
A high index of suspicion should be used in snowboarders who complain of lateral ankle pain with a normal-appearing ankle radiograph. Computed tomography imaging is often required to diagnose a talus fracture.
Hyperplantarflexion variant ankle fracture
This fracture is composed of a posterior tibial lip fracture with posterolateral and posteromedial fracture fragments separated by a vertical fracture line. The ankle fracture “spur sign” is peculiar. The spur sign is a double cortical density at the inferomedial tibial metaphysis.
Laboratory Studies
No laboratory studies are generally required. A workup for osteoporosis, Charcot-Marie-Tooth disease, arthritis, connective tissue disease, or peripheral vascular disease may be done in recurrent fractures
Imaging Studies
See Ottawa rules for ankle radiography
Anteroposterior [AP], lateral, and mortise views of the ankle are generally sufficient for ankle injuries. In the mortise view, the foot is rotated approximately 15° internally, allowing better visualization of the ankle mortise.
CT and MRI imaging studies may be part of outpatient management where imaging features by the other modalities are equivocal.
A bone scan may be useful for diagnosing and localizing stress fractures, infections, and neoplastic lesions.
Treatment of Ankle Injuries
Patients with ankle injuries must be evaluated for further trauma.
Ankle fracture should be identified as stable or unstable.
Unstable fractures are
- Any fracture-dislocation
- Bimalleolar or trimalleolar fractures
- Lateral malleolar fracture with significant talar shift.
If the neurovascular status of the extremity is compromised, the fracture should be reduced as soon as possible and further course of the treatment depends on the response.
Open fractures should be aggressively treated by wound lavage, sterile dressing, antibiotics, tetanus immunoglobulin/prophylaxis
Ankle splints are commercially available or may be constructed by sandwiching 10-12 layers of plaster between 4 sheets of cotton padding.
The splints used maybe a posterior splint or sugar tong splints.
Definitive treatment
Undisplaced fractures are treated with splinting and plaster cast application.
Displaced fractures often require surgery for anatomical reduction and fixation. The approaches to the treatment would vary according to the fracture and are discussed separately under the individual groups of fractures.
Complications
Prognosis
The prognosis is good with prompt, accurate diagnosis and appropriate treatment and referral.
Complex open fractures have a worse prognosis than isolated closed ankle fractures.
Orthotics and proper shoe gear may help prevent future injury.
References
- Shariff SS, Nathwani DK. Lauge-Hansen classification–a literature review. Injury. 2006 Sep. 37(9):888-90.
- Duchesneau S, Fallat LM. The Tillaux fracture. J Foot Ankle Surg. 1996 Mar-Apr. 35(2):127-33; discussion 189
- Dowdall H, Gee M, Brison RJ, Pickett W. Utilization of radiographs for the diagnosis of ankle fractures in Kingston, Ontario, Canada. Acad Emerg Med. 2011 May. 18(5):555-8.
- Gonzalez O, Fleming JJ, Meyr AJ. Radiographic Assessment of Posterior Malleolar Ankle Fractures. J Foot Ankle Surg. 2014 Sep 25.
- Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures–an increasing problem?. Acta Orthop Scand. 1998 Feb. 69(1):43-7.
- Werner CM, Lorich DG, Gardner MJ, et al. Ankle fractures: it is not just a “simple” ankle fracture. Am J Orthop. 2007 Sep. 36(9):466-9