Last Updated on October 29, 2023
Ankylosing spondylitis literally means fusing inflamed spine growing together.
Ankylosing spondylitis is also known by many other names like rheumatoid spondylitis spondyloarthrite rhizomegalique,Marie-Strümpell disease and von Bechterew disease.
Ankylosing spondylitis is a chronic inflammatory joint disease which is a part of spondyloarthropathies. Reactive arthritis, psoriatic arthropathy, spondyloarthropathy associated with inflammatory bowel disease, undifferentiated spondyloarthropathy, Whipple disease, and Behcet disease are other types of spondyloarthropathies.
Ankylosing spondylitis is the most prevalent of the classic spondyloarthropathies
[Read more on spondyloarthropathies]
Ankylosing spondylitis primarily affects axial skeleton, usually begins in adolescence and early adulthood. The disease also affects peripheral joints as well, hip and shoulder being most common.
The prevalence of ankylosing spondylitis is 0.1-0.2% and may be higher in certain populations.
HLA-B27 and ankylosing spondylitis are higher in whites and certain Native Americans than other populations.
The male-to-female ratio of ankylosing spondylitis is 3:1.
Pathophysiology of Ankylosing Spondylitis
Ankylosing spondylitis and other spondyloarthropathies are chronic inflammatory diseases affecting the sacroiliac joints, axial skeleton, and, peripheral joints. These also affect organs other than joints like the eyes, skin, and cardiovascular system. The cause is not known but involves the interaction of genetic and environmental factors.
The spondyloarthropathies are associated strongly with HLA-B27, an HLA class-I gene.
Entheses are the sites where tendons and ligaments insert. Inflammation of entheses is a hallmark of ankylosing spondylitis and other spondyloarthropathies.
CD4+ and CD8+ T lymphocytes, macrophages, cytokines such as TNF-? and transforming growth factor-?, are important in the inflammatory mediators.
Inflammation leads to fibrosis and ossification at the site of enthesitis.
Genetic predisposition
Some people are genetically susceptible. Association with HLA-B27 is known. Other genes associated with ankylosing spondylitis include IL-1 gene cluster, CYP 2D6, ANKH and HLA-DRB1.
People who are homozygous for HLA-B27 are at a greater risk for ankylosing spondylitis than those who are heterozygous.
Immunologic mechanisms
The shared amino acid sequence of the HLA-B27 molecule is present in the antigen-binding region. A molecular mimicry is the suggested mechanism where an environmental trigger (Klebsiella) causes presentation of an arthritogenic peptide from enteric bacteria by specific HLA molecules.
Many patients with ankylosing spondylitis have subclinical gastrointestinal tract inflammation and elevated IgA antibodies directed against Klebsiella. The bacteria may invade the gastrointestinal tract of a genetically susceptible host, leading to chronic inflammation and increased permeability. Over time, bacterial antigens containing arthritogenic peptides enter the organism via the bloodstream.
Localization of pathology to certain types of connective tissues (eg, entheses) may be explained by the affinity of bacterial antigens to these specific sites probably due to biomechanical stress.
Environmental factors
Ankylosing spondylitis does not develop in every person who is HLA-B27 –positive, indicating that environmental factors are important.
Spectrum and Progression of Disease in Ankylosing Spondylitis
The disease begins in the sacroiliac joints. Most patients have a mild chronic disease or intermittent flares with periods of remission. Progression occurs from the lumbosacral region to involve other regions of the spine.
Peripheral involvement is seen in 30-50% of the patients.
The disease causes inflammation at the site of insertion of ligaments and tendons on to the bone. It is termed as peripheral enthesitis.
This often progresses from erosion and osteitis to ossification, resulting in telltale radiological signs of periosteal new bone formation.
Common sites of enthesitis are
- Achilles tendon insertion
- Plantar fascia insertion on the calcaneus or the metatarsal heads
- Base of the fifth metatarsal head,
- Tibial tuberosity
- Superior and inferior poles of the patella
- Iliac crest
- Greater trochanter
- Ischial tuberosity
- Costochondral junctions
- Distal scapula
- Lateral epicondyle
- Distal ulna.
Other Systems involvement
- Uveitis is the most common extra-articular manifestation [20-30% ]. Uveitis associated with other spondyloarthropathies
- Cardiovascular involvement <10% of patients, typically those with severe long-standing disease.
- Restrictive lung disease may occur in patients with late-stage ankylosing spondylitis. Costovertebral and costosternal involvement lead to limited chest expansion.
- Amyloidosis is very rare. This may result in renal dysfunction with proteinuria and renal insufficiency or failure.
- Neural complications secondary to fractures of a fused spine
- Asymptomatic inflammation of the proximal colon and terminal ileum has been observed in about 60%
- Osteopenia and osteoporosis
Clinical Presentation of Ankylosing Spondylitis
Ankylosing spondylitis primarily affects axial skeleton, usually begins in adolescence and early adulthood. The course of the disease is characterized by remissions and exacerbations.
Clinical presentation of ankylosing spondylitis varies from individual to individual.
The symptoms are related to inflammatory back pain, peripheral enthesitis, arthropathy, and constitutional and extra-articular involvement. Systemic symptoms like fever and weight loss may and fatigue is may occur. Morning stiffness is characteristic.
Inflammatory back pain
Inflammatory back pain is most common presenting feature which about 75% people present with.
Inflammatory back pain ha following features
- Insidious onset
- > 3 months of symptoms before presentation
- Morning stiffness lasting at least 30 minutes, improvement of symptoms with moderate physical activity
- Diffuse nonspecific radiation of pain into both buttocks
- Patients may wake up in the morning with pain and stiffness
More on inflammatory back pain
Peripheral Pains
Pain at the site of enthesitis like the back of the heel [Achilles tendon insertion], heel [plantar fasciitis] occurs in 30-50% of the cases.
Pain is reported mainly in the hips, shoulders, and joints of the chest wall, including the acromioclavicular and sternoclavicular joints. Other peripheral joints are involved less frequently and to a milder degree.
The examination may reveal tenderness of the sacroiliac joints and a stiff spine. In later stages, kyphosis resulting in a stooped posture, typical of ankylosing spondylitis, may be noted.
Schober test
This test is done to assess for the range of motion in the spine.
Schober test is performed by marking a 10-cm length of the lumbar spine with a patient in the erect position, starting at the fifth lumbar spinous process. After this, the patient is instructed to flex her spine maximally.
Remeasure the distance between the marks. Normal flexion increases the distance by at least 5 cm.
Chest expansion
Loss of chest expansion (<3-cm difference between a minimum and maximum chest diameter) is usually found only in patients with late-stage disease and is generally not helpful in diagnosis.
Peripheral lesions are tender upon examination and may be associated with swelling. Carefully examine patients for tenderness upon palpation.
Involved joints should be examined for tenderness and restriction of motion. In later stages, deformities of the joint may be seen.
Extraarticular manifestations
These depend on the organ involved
- Uveitis usually presents as an acute red painful red eye with photophobia, increased lacrimation, and blurred vision. An attack lasts about 2-3 months
- Cardiovascular involvement
- Aortitis
- aortic valve insufficiency.
- Mitral valve insufficiency
- Fibrosis of the conduction system may result in various degrees of atrioventricular block
- Bilateral apical pulmonary fibrosis. Sometimes may get infected. Cough dyspnea and hemoptysis may occur
- Renal involvement in amyloidosis may result in urinary symptoms
Other presentations are that of to atlantoaxial subluxation resulting in myelopathy, cauda equina syndrome and rarely Crohn disease or ulcerative colitis
Differential Diagnoses
- Lumbar Disc Disease
- Lumbar Spondylosis
- Psoriatic Arthritis
- Reactive Arthritis
- Inflammatory bowel disease associated spondyloarthropathy
- Juvenile idiopathic arthritis
- Diffuse idiopathic skeletal hyperostosis
Diagnostic Work of Ankylosing Spondylitis
No laboratory tests are specific for ankylosing spondylitis. The diagnosis is made by combining the clinical criteria of inflammatory back pain and enthesitis or arthritis with radiological findings. Two sets of criteria are used for diagnosis of spondyloarthropathies in general.
New York and Rome criteria are used widely for the diagnosis of ankylosing spondylitis.
| New York Criteria (1984) | Rome Criteria (1961) |
| Low back pain with inflammatory characteristics
Limitation of lumbar spine motion in sagittal and frontal planes Decreased chest expansion Bilateral sacroiliitis grade 2 or higher Unilateral sacroiliitis grade 3 or higher |
Low back pain and stiffness for >3 months that is not relieved by rest
Pain and stiffness in the thoracic region Limited motion in the lumbar spine Limited chest expansion History of uveitis |
| Definite ankylosing spondylitis when the fourth or fifth criterion mentioned presents with any clinical criteria | Diagnosis of ankylosing spondylitis when any clinical criteria present with bilateral sacroiliitis grade 2 or higher |
Lab Studies
- Normochromic normocytic anemia of chronic disease may be noticed in about 15%
- Elevated / C-reactive protein 75%
- Raised alkaline phosphatase is elevated in 50% of patients
- Creatine kinase and serum IgA level may be elevated
- Though it has an association, determining HLA-B27 status is not a necessary part of the clinical evaluation.
Imaging Studies
Radiographs
Radiographs often diagnostic but in the very initial period of the disease, the radiographs may entirely be normal as skeletal changes that could be depicted by radiographs come late.
Radiographs show the following features
Sacroiliitis
It is usually bilateral, symmetric, and gradually progress from blurring of the subchondral bone plate to irregular erosions of the margins of the sacroiliac joints to sclerosis, narrowing, and finally fusion.
Erosions of the subchondral bone of the sacroiliac joint are generally seen earlier in the lower portion of the joint.
Spine
Vertebral changes start in the thoracolumbar spine and progress proximally
Early radiographic signs include
- Loss of normal concave contour resulting in square vertebra[due to erosions margins of these bodies]
- Sclerosis of the superior and inferior margins of the vertebral bodies, called shiny corners or Romanus lesion
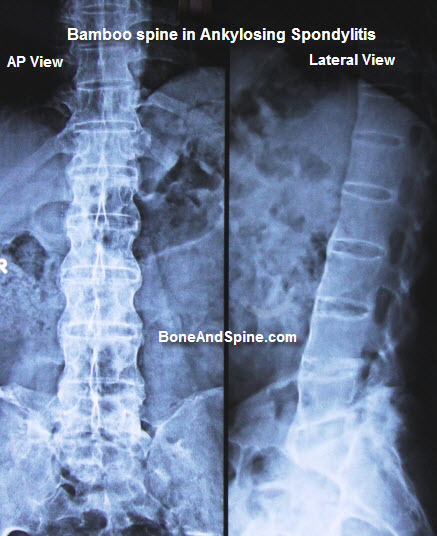
- Ossification of the annulus fibrosus leads to the radiographic appearance of syndesmophytes. Over time, development of continuous (bridging) syndesmophytes may result in a fused spine, also termed as bamboo spine.
Other Regions
- Radiographs of the pelvis may show ossification of the iliac crest, ischial tuberosity, and femoral trochanter [ whiskering]. Occasionally, the symphysis pubis develops erosive changes (osteitis pubis).
- Erosion, periosteal new bone formation, and, ossification, at the insertion of the Achilles tendon and the plantar fascia on the calcaneus.
- Joint space narrowing in hips and shoulders along with degenerative changes. Ultimately, peripheral joints may undergo ankylosis.
- Heterotopic bone formation may occur after total joint replacement, MRI/CT
MRI or CT
MRI/CT may show early sacroiliitis, erosions, and enthesitis that are not apparent on standard radiographs.
These investigations are not routinely done though.
MRI and a CT scan may be useful in the diagnosis of a spinal fracture in patients with late-stage spinal disease.
Treatment of Ankylosing Spondylitis
There is no cure for ankylosing spondylitis. The objectives of the treatment are
- Halting or slowing the disease progression
- Pain relief
- Relief from stiffness and fatigue
- Maintenance of good physical and psychosocial functioning.
Drugs, patient education, cognitive therapy, and exercises are important in patient management.
Medical Treatment of Ankylosing Spondylitis
The patient should be educated about the disease and expectation from the treatment
Drugs
No drugs have been proven to modify the course of the disease, although TNF-alpha antagonists have potential as disease-modifying agents.
Nonsteroidal anti-inflammatory drugs
NSAIDs improve the symptoms of the disease. Indomethacin may be more effective than other NSAIDs, although this has not been proven. Continuous treatment with NSAIDs appears to reduce radiographic progression in ankylosing spondylitis.
Sulfasalazine
Sulfasalazine reduces spinal stiffness, peripheral arthritis, and the ESR, but no evidence shows that spinal mobility, enthesitis, or physical function is benefited.
Toxicities include rash, nausea, diarrhea, and agranulocytosis (rarely).
Newer Drugs
- The TNF-alpha antagonists have been shown to be effective in the treatment of ankylosing spondylitis. Etanercept, infliximab, and adalimumab are frequently used drugs. These agents have been shown to reduce the inflammatory activity of spinal disease as assessed with MRI.
- Bisphosphonates may modestly affect clinical disease activity in ankylosing spondylitis.
- Anakinra is a recombinant human interleukin 1 (IL-1) receptor antagonist which may be effective in treatment-resistant ankylosing spondylitis.
Corticosteroids
Oral corticosteroids are occasionally helpful in controlling symptoms but should be used for short-term only.
Local corticosteroid injections are useful for symptomatic sacroiliitis, peripheral enthesitis, and arthritis, although the response is not typically as rapid as in patients with rheumatoid arthritis.
Extra-articular manifestations are treated as per the presentation.
Physical therapy
Exercise and postural training is important to maintain function.
- Spinal extension and deep-breathing exercises
- Maintain spinal mobility
- Encourage erect posture
- Promote chest expansion.
- Maintain an erect posture during daily activities
- Sleeping on a firm mattress with a thin pillow reduces the tendency toward thoracic kyphosis.
- Water therapy and swimming maintain mobility and fitness.
Surgical Treatment
- Vertebral osteotomy to correct spinal deformities
- Joint replacement surgery for damaged joints. Risk of heterotopic bone formation can be reduced by using postoperative indomethacin
Complications of Ankylosing Spondylitis
- Spinal fusion
- Severe kyphosis
- Limitation of motion of the spine including cervical spine
- Fractures in the fused spine
- Peripheral joint arthropathy
Prognosis
Ankylosing spondylitis though cannot be cured carries overall good prognosis.
Patients often require long-term anti-inflammatory therapy. Morbidity can occur due to spinal and peripheral joint involvement or, rarely, extra-articular manifestations.
Poor prognostic indicators include peripheral joint involvement, young age of onset, elevated ESR, and poor response to NSAIDs.
The risk of mortality is increased in patients with ankylosing spondylitis who have a severe long-standing disease and significant extra-articular manifestations.
Because of the joint involvement in the chest wall and the potential for pulmonary complications, include smoking cessation in recommendations.
Juvenile Ankylosing Spondylitis
Juvenile ankylosing spondylitis is clinically similar to adult ankylosing spondylitis.
In about 10-20% of all cases, onset occurs before age 16 years. Just like adult ankylosing spondylitis, the male-to-female ratio is.
Enthesitis is prominent early in the course of the disease, while spinal symptoms and limitation of motion may not be present until several years later. This feature is in contrast to the adult pattern.
Peripheral arthritis and dactylitis are more common, especially in lower limbs.
Systemic involvement is more common. Features like fever, weight loss, anemia, leukocytosis are more common.
Making a diagnosis with certainty is difficult as X-rays of pelvis and spine are difficult to interpret in children and are often normal.