Last Updated on August 2, 2019
Anterior interosseous nerve syndrome or Kiloh-Nevin syndrome is neuropathy of the anterior interosseous nerve, a motor branch of the median nerve, that results in pain in the forearm and a characteristic weakness of the thumb and index finger.
Though most of the cases of anterior interosseous nerve syndrome are due to a transient neuritis, similar to Parsonage-Turner syndrome. Compression or trauma of the nerve can be a cause of the symptoms.
AIN syndrome is now regarded as a neuritis (inflammation of the nerve) in most cases; this is similar to Parsonage-Turner syndrome.
Cause of the condition is not known but thought to be an immune-mediated response.
Relevant Anatomy

The anterior interosseous nerve is a terminal motor branch of the median nerve which arises 4-6 cm distal to the medial epicondyle
It travels between flexor digitorum superficialis and flexor digitorum profundus initially, then between flexor pollicis longus and flexor digitorum profundus.
Then it lies on the anterior surface of the interosseous membrane traveling with the anterior interosseous artery
Terminal branches innervate the joint capsule and the intercarpal, radiocarpal and distal radioulnar joints.
Anterior interosseous nerve has principally motor supply innervates
- Flexor digitorum profundus to index and middle finger)
- Flexor pollicis longus
- Pronator quadratus
Causes of Anterior Interosseous Nerve Syndrome
The anterior interosseous branch of the median nerve is subject to compromise near its origin. This syndrome usually occurs spontaneously, but can be caused by fracture, fibrous bands, aberrant or thrombosed vessels, and tumors.
Known sites of compression include the following:
- Gantzer’s muscle
- Accessory head of the flexor pollicis longus
- Found to be posterior to both the median nerve and the anterior interosseous nerve in all cases
- Fibrous arch of the flexor digitorum superficialis
- Fascial bands of the deep head of the pronator teres
- Aberrant palmaris profundus
- Aberrant flexor carpi radialis brevis
- Edge of lacertus fibrosus
- Accessory muscle from flexor digitorum superficialis to flexor digitorum profundus
- Aberrant muscles (Flexor carpi radialis brevis, palmaris profundus)
- Thrombosed ulnar-radial or ulnar artery
- Gruber anastomoses
- Anomalous anatomy in 15% of the population
- Axons of the anterior interosseous nerve may cross over and connect to ulnar nerve and innervate other muscle groups
Presentation
Patients typically present with motor weakness. There is generally no complaints of pain [compare with other median compression neuropathies (carpal tunnel syndrome and pronator syndrome)
There would be the inability to flex the terminal phalanges of the thumb and index finger (eg, loss of pinch and fine motor skills such as writing) and the inability to pronate the forearm when the elbow is flexed.
There is a weakness of the flexor pollicis longus, the flexor digitorum profundus of the index finger, and the pronator quadratus.
There is typically no sensory deficit.
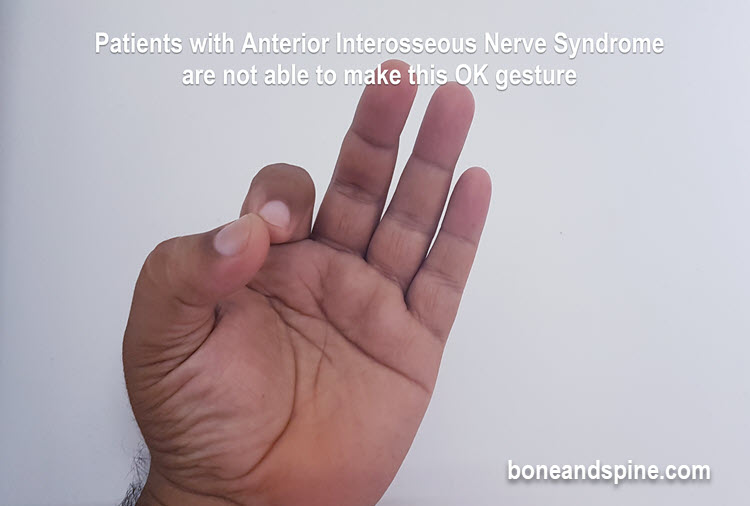
Patient unable to make OK gesture [requires functional flexor digitorum and flexor pollicis longus].
Following is an ok gesture
Pronator quadratus weakness is revealed by resisted pronation with elbow maximally flexed
Passive wrist extension brings thumb interphalangeal joint and index finger distal interphalangeal joints into relatively flexed position.
Differential Diagnoses
- Parsonage-Turner Syndrome
- Viral brachial neuritis
- Flexor tendon rupture.
Diagnosis
NCV / EMG
These studies may reveal abnormalities in the flexor pollicis longus, flexor digitorum profundus of index finger and middle finger and pronator quadratus muscles
These studies are helpful to make a diagnosis and assess the severity of neuropathy. They are also helpful in ruling out out more proximal lesions
Treatment
Majority of the patients are treated with nonoperative treatment which includes observation, rest and splinting in 90° flexion.
The treatment is continued for 8-12 weeks.
Operative is indicated when nonoperative treatment fails after several months. It is also indicated if there is a clear space-occupying mass.
Surgery involves decompression of anterior interosseous nerve which is accomplished by
- The release of the superficial arch of FDS and lacertus fibrosus
- The detachment of superficial head of pronator teres
- Ligation of any crossing vessels
- Removal of any space occupying lesion