Last Updated on December 25, 2023
Atlanto-occipital fusion or Occipitalization of the atlas [C1 vertebra]is the most common congenital abnormality of the upper cervical spine. It means partial or complete congenital fusion between the atlas and the base of the occiput.
Other names for atlanto-occipital fusion are occipitalization, occipitocervical Synostosis, assimilation of Atlas.
The severity ranges from a complete bony fusion to a bony bridge or even a fibrous band. Occipitalization occurs because of failure of segmentation between the fourth occipital sclerotome and the first spinal sclerotome.
The incidence has been reported to be 1.4 to 2.5 per 1000 children. It affects both sexes equally.
Being typically asymptomatic, the atlanto-occipital fusion can remain unnoticed and be found incidentally on imaging/autopsy.
Atlanto-occipital fusion was first described by Rokitansky in 1844, and Schuller in 1911. It was earlier called proatlas as it was thought that there is an additional vertebra between the atlas and occipital bone.
Reevant Anatomy and Pathophysiology
Atlas is the first cervical vertebra that sits just below the skull. It is also called C1 vertebra. Atlas is unique in its shape. It articulates with the dens of the axis, an upward projection of axis or C@ vertebra.
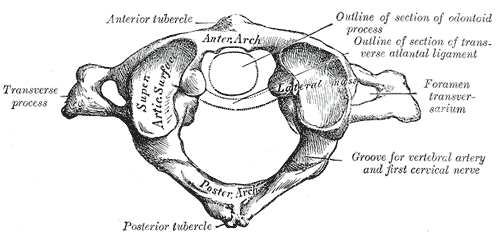
Atlas can be identified by its ring shape. There is no vertebral body or spinous process.
The atlas is composed of
- Anterior arch – forms one fifth of the ring.
- Posterior arch – Forms three-fifths of the ring
- Paired lateral masses
- Paired transverse processes
Fusion between atlas and occipital bone occurs is mainly between the arch and rim of the foramen with small part of the posterior arch involved. The fusion may involve both lateral masse
Manifestations of atlanto-occipital fusion condition are mainly attributed to the ligamentous laxity of the transverse ligament and flexion-extension movements of neck causing compression of the cord. Repeated injuries to the nerves from the odontoid may result in the neurological symptoms.

Associated Conditions
- Fusion C2 and C3 (50-70%)
- Kyphosis & scoliosis
- Anomalies of the jaw
- Incomplete cleft of the nasal cartilage
- Cleft palate
- External ear deformities
- Cervical ribs
- Urinary tract anomalies
- Basilar invagination
- Craniocervical instability
Symptoms and Signs
Patients with atlanto-occipital fusion may have have
- Low hairlines
- Torticollis
- Short necks
- Headaches that are worsened by strain, coughing, sneezing or bending
- Dull pain in the neck and posterior skull
- Episodic neck stiffness
Neurological symptoms usually occur in third and fourth decades and vary depending on the area of spinal cord impingement and can cause (including those of due to cranial nerve involvement)
- Limbs
- Numbness
- Pain
- Weakness
- Tinnitus
- Distrubances of vision
- Dysphgia (difficulty in eating)
- Dysarthria (difficulty in speaking)
- visual disturbances and lower cranial nerve palsies leading to dysphagia and dysarthria.
Nystagmus is a common finding.
Cranial nerve involvement can cause diplopia, dysphagia, and auditory disturbances.
Vertebral artery involvement may result in syncope, seizures, vertigo, and an unsteady gait.
Radiographic Findings
Routine radiographs usually are difficult to interpret, and CT scan or MRI may be needed to show the occipitocervical fusion. Most commonly, the anterior arch of the atlas is assimilated into the occiput and displaced posteriorly relative to the occiput.
About half of patients of atlanto-occiptal fusion have a relative basilar impression due to loss of height of the atlas.
Posterior fusion usually is a small bony fringe or a fibrous band that frequently is not evident on a radiograph.
Atlantoaxial instability should be looked for by flexion and extension views of the neck.
Myelography or MRI can detect areas of encroachment on the spinal cord or medulla
Treatment of Atlanto-occipital Fusion
Patients of atlanto-occipital fusion who have minor symptoms or become symptomatic after minor trauma or infection can be treated conservatively with immobilization in plaster, traction, or a cervical orthosis.
When neurological symptoms occur, cervical spine fusion or decompression is indicated.
Anterior symptoms usually are caused by a hypermobile odontoid, therefore preliminary reduction of the odontoid with traction, followed by fusion from the occiput to C2, relieves the symptoms.
If the odontoid is irreducible, excision of the odontoid may be taken.
Posterior signs and symptoms usually are caused by bony compression or compression from a dural band. Removal of the dural band is indicated when a band is documented by CT or MRI. Posterior fusion may be added to prevent instability.
References
- AL-Motabagani MA, Surendra M. Total occipitalization of the atlas. Anatomical Science International. 2006;81(3):173–80. [Link]
- Monika L, Sanjay P, Anupama M, Kullar JS. Occipitalization of atlas: A case report with its ontogenic basis and review of literature. Current Trends in Diagnosis and Treatment. 2017;1(1):34–37.