Last Updated on October 29, 2023
The pelvic region of the trunk is the lower part of the trunk, between the abdomen and the thighs. It includes the following structures. Bony pelvis or pelvic skeleton is formed by hip bones, sacrum, and coccyx.
Anatomy of the pelvis includes anatomy of the bony pelvis and its contents. In this article, we would discuss bony pelvis.
Anatomy of Bony Pelvis
The pelvis is a ring structure made up of three bones: the sacrum and two innominate bones. The three bones and three joints composing the pelvic ring have no inherent stability without vital ligamentous structures.
The bony pelvis is formed posteriorly by the sacrum and the coccyx and laterally and anteriorly by a pair of hip bones.
Joints of Pelvis
Lumbosacral joint
This joint is between the sacrum and the last lumbar vertebra [L5]. It allows flexion and extension and a small amount of lateral flexion. It includes an intervertebral disc and joints between the articular processes.
In children, this joint contributes as much as 75% of flexion and extension in the lumbar spine but decreases considerably after that.
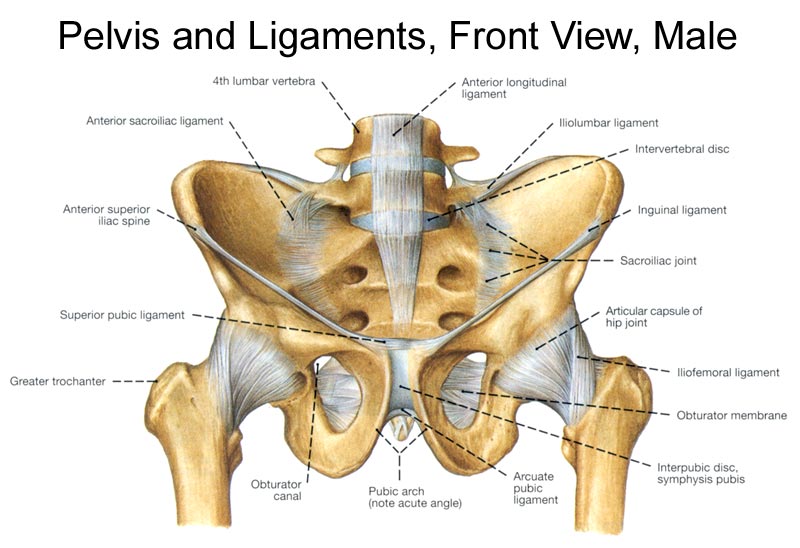
Apart from intervertebral supports, the lumbosacral joint is enhanced in strength by the iliolumbar ligament that extends from transverse process of L5 to iliac crest.
Sacrococcygeal joint
It is a secondary cartilaginous joint consisting of an intervertebral disc between the sacrum and coccyx and accessory ligaments. This joint may fuse with age.
The anterior sacrococcygeal ligament is an extension of the anterior longitudinal ligament.
The posterior sacrococcygeal ligament has a deep part, an extension of the posterior longitudinal ligament and a superficial part corresponding to the ligamenta flava [also called yellow ligament].
Sacro-iliac Joints
Sacro-iliac joints are synovial joints between the auricular surfaces of the sacrum and ilium on each side.
Sacroiliac joints are almost immobile joints enclosed by very taut joint capsules attached closely to articular margins.
The sacroiliac joint is made up of two parts. The caudal portion consists of the articular surface of the joint; the upper, more dorsal portion, between the posterior tuberosity of the ilium and the sacrum, contains the fibrous or ligamentous parts of the joint (interosseous ligaments).
The joint is strengthened by following ligaments
Ventral sacroiliac ligament
It is thickening of anterior and inferior parts of the fibrous capsule. Its lower part is attached to preauricular sulcus.
Interosseous sacroiliac ligament
It is a large and strong ligament which connects wide, rough areas adjoining concave margins of the auricular surfaces. It is covered by dorsal sacroiliac ligament.
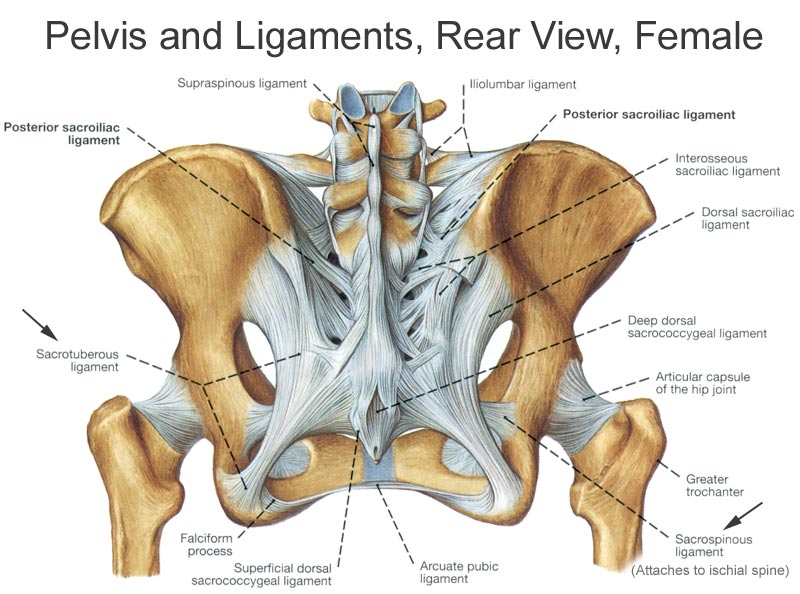
Dorsal sacroiliac ligaments
It covers the interosseous sacroiliac ligament and from that, it is separated by dorsal rami of sacral nerves, and vessels.
This ligament consists of
- Short transverse fibers [short posterior sacroiliac ligament] that pass from ilium to the transverse tubercle of first two sacral vertebrae.
- Long, vertical band [long posterior sacroiliac ligament] from posterior superior iliac spine to transverse tubercle of 3rd and 4th sacral pieces. It is continuous laterally within the medial edge of sacrotuberous ligament.
Iliolumbar ligament
It is a strong triangular ligament which extends from transverse process of L5 to posterior part of the inner lip of iliac crest. It is continuous with the middle and anterior layer of thoracolumbar fascia and also gives partial origin to the quadratus lumborum. It is covered anteriorly by psoas muscle and posteriorly by erector spinae. Its main function is to prevent anteroinferior slipping under body weight. It also limits the forward movement at sacroiliac joint.
The lateral lumbosacral ligament is partly continuous with the iliolumbar ligament. It passes between the transverse process of the fifth vertebra to the ala of the sacrum where it intermingles with the anterior sacroiliac ligament.
Sacrotuberous Ligament
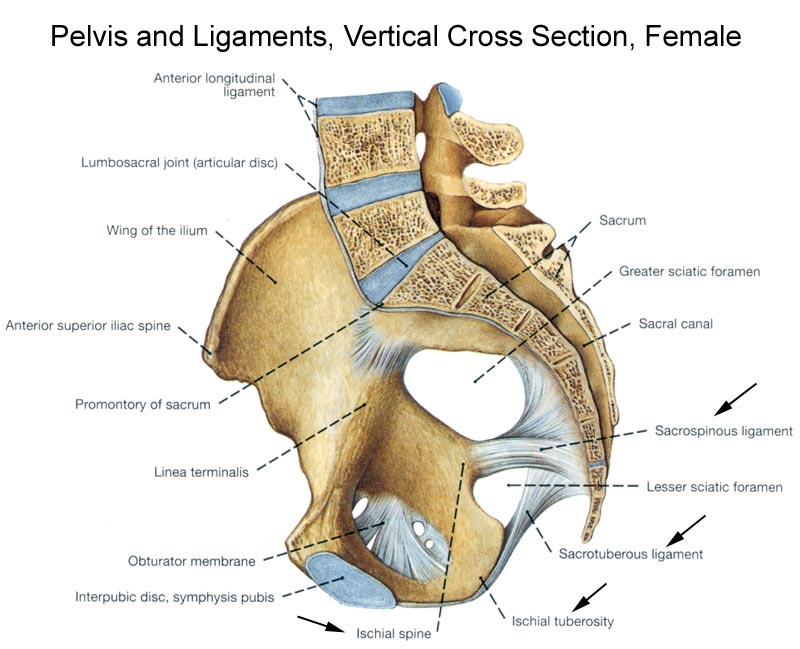
This ligament, along with sacrospinous ligaments stabilize the hip bone on the sacrum and prevent the promontory from tilting forward. Additionally, these two ligaments transform the greater and lesser sciatic notches into the greater and lesser foramina, a pair of important pelvic openings. [The sacrotuberous ligament converts the sciatic notches into foramina, which are separated from each other by the sacrospinous ligament.]
Sacrotuberous ligament extends as wide base from the dorsal surface of the sacrum [lower transverse tubercles of the sacrum and lateral margin of the lower part of sacrum], the upper part of the coccyx, posterior superior and inferior iliac spine the ilium and coccyx and to the medial margin of the ischial tuberosity. It converts lesser and greater sciatic notches into foramina and forms the lateral boundary of pelvic outlet.
The sacrospinous ligament lies deep to sacrotuberous ligament extends from the lateral margin of the sacrum (and coccyx) to the ischial spine. Morphologically, the ligament is considered to be a degenerated part of the coccyx.
The greater sciatic foramen transmits the piriformis muscle, superior and inferior gluteal vessels and nerves, (internal) pudendal vessels and nerve, sciatic and posterior femoral cutaneous nerves, and the nerves to the obturator internus and quadratus femoris muscles.
The lesser sciatic foramen transmits the obturator internus tendon, the nerve to the obturator internus, and the (internal) pudendal vessels and nerve.
Iliolumbar, sacrotuberous and sacrospinous ligaments are together called vertebropelvic ligaments.
Pubic symphysis
It is a cartilaginous joint between the bodies of the pubic bones.. The symphysial surfaces, each covered by hyaline cartilage, are united by an interpubic disc of fibrocartilage. The disc is reinforced by surrounding ligamentous fibers.
Pubic symphysis permits slight movement between hip bones which help in absorbing shocks.
Pelvic Cavity
The pelvic cavity is a body cavity that is bounded by the bones of the pelvis and which primarily contains reproductive organs and the rectum.
A distinction is made between the lesser or true pelvis inferior to the terminal line, and the greater or false pelvis above it.
Area between the pelvic inlet [also called superior pelvic aperture and is bordered by the promontory, the arcuate line of ilium, the iliopubic eminence, the pecten pubis, and the upper part of the pubic symphysis] and pelvic outlet [also called inferior pelvic aperture and bordered by the or pubic arch [subpubic angle, the ischial tuberosities and the coccyx] is called lesser or true pelvis.

The inlet is at about 45 degrees of angle to the horizontal.
The greater pelvis or false pelvis is the space enclosed by the pelvic girdle above and in front of the pelvic inlet.
Pelvic Floor
The pelvic floor functions to close the pelvic and abdominal cavities and bear the load of the visceral organs. It also controls the openings of the rectum and urogenital organs.
The pelvic diaphragm is composed of the levator ani and the coccygeus muscle [arising from symphysis and the ischial spine and converge on the coccyx] and the anococcygeal ligament [between the tip of the coccyx and the anal hiatus]. This leaves a slit for the anal and urogenital openings. The urogenital diaphragm is reinforced posteriorly by the superficial transverse perineal.
The wall of the pelvic cavity includes superficial muscles, such as the glutei, the hip bones, the sacrum and coccyx, and their associated ligaments, deep muscles, blood vessels, nerves, and peritoneum.
Gender Variation in Bony Pelvis
The principal differences between male and female true and false pelvis include:
- The female pelvis is larger and broader as compared to taller, narrower, and compact male pelvis.
- The female inlet is larger and oval in shape whereas the male inlet is heart shape because the male sacral promontory projects forward.
- In the male pelvis, sides converge from the inlet to the outlet, whereas the sides of the female pelvis are wider apart. This makes the distance between the ischial bones is lesser in males. The greater sciatic notch is wider in females.
- The iliac crests are higher and more pronounced in males and the male sacrum is long, narrow, more straight.
- The acetabula are wider apart in females than in males. In males, the acetabulum faces more laterally, while it faces more anteriorly in females. Consequently, when men walk the leg can move forwards and backwards in a single plane. In women, the leg must swing forward and inward, from where the pivoting head of the femur moves the leg back in another plane. This change in the angle of the femoral head gives the female gait is characteristic swinging of hips.
Stability of Pelvis
Ligaments of the pelvis provide it the required stability.
The posterior sacroiliac ligaments form a posterior tension band for the pelvis.
Transverse ligaments, like the short posterior sacroiliac and the anterior sacroiliac ligaments along with the iliolumbar and sacrospinous ligaments, resist rotational forces.
Vertical ligaments like long posterior sacroiliac, sacrotuberous, and lateral lumbosacral ligaments resist vertical shear.
Neurovascular structures
The common iliac blood vessels enter into the false pelvis, in which the division into the external and internal iliac vessels occurs. The external iliac vessels continue through the false pelvis atop the pubic rami medial to the iliopectineal eminence. The internal iliac vessels dive into the pelvis, in which they divide into somatic branches [iliolumbar, lateral sacral], visceral branches [umbilical, inferior vesicle, superior vesicle, middle rectal] and limb and perineal branches [Superior & inferior gluteal, internal pudendal and obturator].
Terminal branch of the aorta, the median sacral artery, and the superior rectal artery [a continuation of the inferior mesenteric artery] also travel to the pelvis.
The neurological contents of the pelvis collectively have been referred to as the lumbosacral plexus which is discussed separately.
Functions of Pelvis
The skeleton of the pelvis is a basin-shaped ring of bones connecting the vertebral column to the femora.
The weight of the body is transmitted through the sacrum and ilia to the femora during standing and to the ischial tuberosities in sitting.
The primary function of the pelvis is to bear the weight of the upper body when sitting and standing, transferring that weight from the axial skeleton to the lower appendicular skeleton when standing and walking, and providing attachments for and withstanding the forces of the powerful muscles of locomotion and posture. It also protects the pelvic and abdominopelvic viscera, provides attachment for external reproductive organs, associated muscles, and membranes.
Image Source
edoctoronline.com