Last Updated on September 26, 2019
Bunion is a bony bump, often painful, enlargement of bone or tissue around the joint at the base of the big toe (metatarsophalangeal joint).
Bunion is a foot deformity, usually associated with hallux valgus [hallux refers to the great toe, “valgus” refers to the abnormal angulation of the great toe], a deformity of the toe where big toe may turn in toward the second toe.
This leads to formation of painful bump on medial aspect of great toe. The bump could be due to the swollen bursal sac and/or bony deformity.
The word “bunion” is derived from the Greek word for turnip as inflamed bump looks like a turnip.
Thus, the bunion is a secondary condition that is formed due to the primary condition – hallux valgus
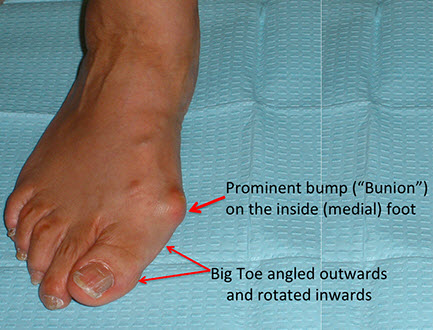
Image Credit: Massgeneral
Hallux valgus and bunion deformity has
- First-phalanx abduction and pronation
- First-metatarsal (MT) adduction, pronation, and elevation
- Capsular and ligamentous derangement.
Relevant Anatomy
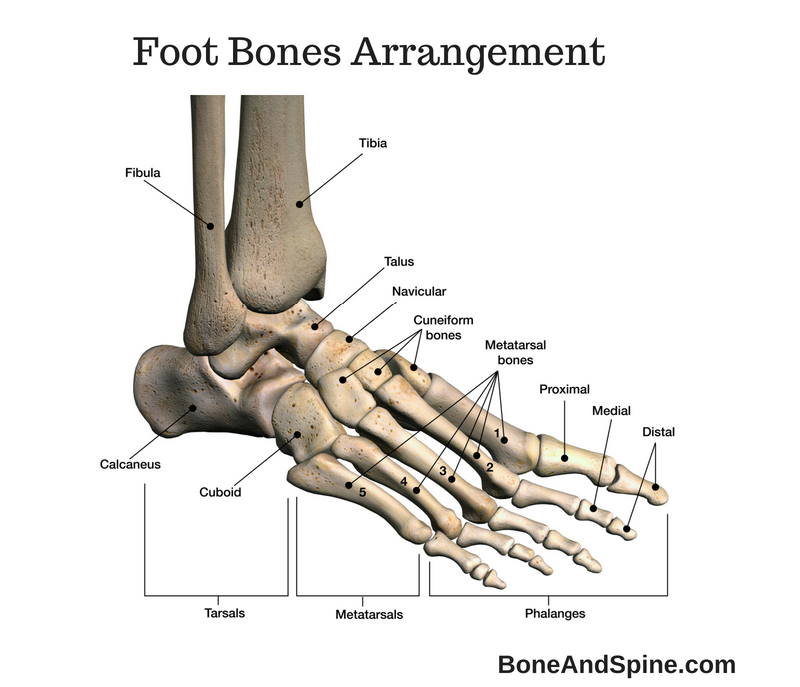
Metatarsophalangeal Joint
The main structure involved is the first metatarsophalangeal joint but interphalangeal joint, the first metatarsocuneiform joint, the hindfoot, and the ankle.
The first metatarsophalangeal joint is formed by
- Metatarsal head
- Proximal phalanx base
- Medial and lateral sesamoids.
A more rounded first metatarsal head is more unstable than the flatter one.
The joint is stabilized by structures around it. The stability of the joint is discussed in the next section along with pathophysiology.

Further here we will discuss various measurements which are important for classifying and planning treatment of hallux valgus
Distal metatarsal articular angle or DMAA
This angle describes the lateral slope of the articular surface of the first metatarsal. This is the angle formed by the intersection of a line along the long axis of the metatarsal and a line along the joint surface of the MT.
Normal value is less than 10 degrees.
Proximal phalanx articular angle
This is a similar angle on the phalangeal side of metatarsophlangeal joint. It is the angle formed by the intersection of a line along the long axis of the proximal and a line along the proximal joint surface of the proximal phalanx. It varies normally from 7 to 10 degrees.
Metatarsophalangeal joint congruence
The lines drawn parallel to the joint surface of both the Pproximal phalanx and the first metatarsal head. The lines are usually parallel. Non parallel lines depict non congruent joint.
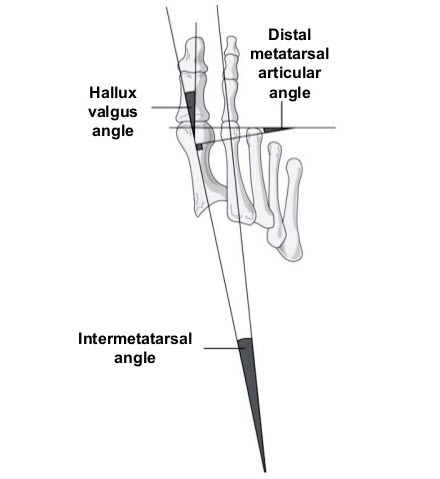
Hallux valgus angle
The hallux valgus angle is formed by the intersection of the lines along the long axis of the proximal phalanx and the first metatarsal [see image]. The normal angle is less than 15 degrees.
Intermetatarsal angles
The angle formed by the intersecting long axis lines along the first and second metatrsals. Normally, this angle should be less than 9 degrees.
Metatarsocuneiform joint
This join is formed by base of the metatarsal and medial cuneiform. If this joint is excessively oblique, it causes hypermobility of the first metatarsal joint.
Sesamoids
Sesamoids or sesamoid bones are located in the flexor hallucis brevis tendon and under the first metatarsal head. They improve the biomechanical axis of the flexor hallucis brevis action.
Crista is the ridge on the plantar aspect of the first metatarsal head which is intersesamoid ridge [Please see the image in metarsophalngeal joint section] in its center, termed the crista.
Normally, the sesamoids are centered under the first metatarsal head when seen in AP view but the subluxation occurs when the first metatarsal head displaces medially.
Balance of Metatarsophalangeal Joint
The balance at the metacarpophalangeal joint is maintained by four groups of muscles and tendons that cross it and attach on the proximal aspect of the proximal phalanx.
- Dorsally
- Extensor hallucis longus and extensor hallucis brevis
- Insert centrally on the distal and proximal phalanges, respectively.
- A ligament called hood ligament keeps them centered.
- Plantar side
- Flexor hallucis longus runs in between the sesamoids
- Inserts on the distal phalanx.
- Gives slips to both sesamoids
- Sesamoids are also connected to proximal phalanx through the plantar plate.
- Medially
- Abductor hallucis tendon inserts on the plantar and medial aspect of proximal phalanx medial aspect of the joint capsule
- Laterally
- Adductor hallucis tendon inserts onto the lateral sesamoid and plantar lateral joint capsule.
Why does Bunion Develop?
For normal alignment of the toe, musculotendinous forces must act in a balanced fashion.
When there is an imbalance in tendons, ligaments, and supportive structures of the first metatarsal do not function correctly and lead to deformity.
Hallux valgus, the primary deformity responsible for bunion can occur in any person and the cause is not known.
Footwear has been implicated as a cause. It is said that pressure on the big toe joint causes the big toe to lean toward the second toe.
Bunions are more common in women, probably due to higher use of more tight, narrow shoes that squeeze the toes together.
There are various conditions associated. These are
- Flat feet
- Hypermobile Joints and Benign Joint Hypermobility Syndrome [Excessive ligamentous flexibility]
- Abnormal bone structure,
- Certain neurological conditions
Bunions sometimes develop in both feet.
Anatomically, bunions develop at the medial aspect of the metatarsophalangeal joint which is a joint between metatarsal and proximal phalanx. It could be a bursa or callosity.
In the beginning, a bunion is small but gets worse over time. As it becomes bigger, it becomes more painful.
In severe bunions, the tip of the big toe may reach the second toe. Their rubbing causes additional discomfort and difficulty walking.
In some cases, enlarged bursitis may occur at the joint.
Bunions in adolescent are also known and often has genetic causes.
Bunion on the outside of the foot near the base of the little toe is called bunionette and is often found in the tailors.
Pathophysiology of Hallux Valgus and Bunion
Lateral deviation of the toe is the primary deformity.
Other changes that occur over the time are
- Pronation of the great toe
- Subluxation/dislocation of the first metatarsophalangeal joint
- An excessive valgus tilt of the articular surface of the first metatarsal head and proximal phalangeal articular surface
- Lateral dislocation of sesamoids occurs as the condition progresses.
There is a natural tendency to pull proximal phalanx in valgus because adductor muscle is stronger than abductor hallucis but under normal circumstances it is well checked.
Initially, medial supporting structures of metatarsophalangeal joint,medial collateral ligaments and medial sesamoid fail. After these structures have failed, the metatarsal head moves medially, beyond and without the sesamoids.
This results valgus position of first proximal phalanx.
The medial sesamoid cause erosion of cartilage on the plantar aspect of head and crista due to friction resulted from new positioning
Increased pressure over the bursa over the medial aspect of the joint can can cause its thickening, forming the bunion.
The pull of the adductor hallucis becomes the primary deforming force as the hallux valgus increases. The pull results in pronation too.
Pronatory rotation effectively removes medial pull of abductor hallucis by making more plantar.
Thus medial check balance is further lost, leaving the job of restraining to the medial capsule, which becomes attenuated over the period.
As the deformity increases, the extensor hallucis longus and brevis, which are no more centered now, bowstring across the lateral side of the deformity, causing further imbalance.
Causes
- Poorly fitting shoes especially those with a narrow tight toe box
- Genetic causes
- Inflammatory condition like rheumatoid arthritis
- Neuromuscular condition, such as polio
Classification of Hallux Valgus Deformity
Mild
- Hallux valgus angle < 20 degrees
- Intermetatarsal angle < 11 degrees
- lateral sesamoid subluxation as seen on AP view < 50 percent
Moderate
- Hallux valgus angle – 20-40 degrees
- Intermetatarsal angle – less than 15 degrees
- Lateral sesamoid subluxation as seen on AP view – 50-75 percent
Severe
- Hallux valgus angle – >40 degrees
- Intermetatarsal angle – >15 degrees
- Lateral sesamoid subluxation as seen on AP view – 50-75 percent
What are the Symptoms of Bunion?
- Pain and tenderness
- Footwear fitting problems
- Irritation of the skin due to excessive pressure from footwear causing hardened skin on the bottom of the foot or callus on the bump
- Restricted motion of the big toe
- Painful walking
Treatment
The diagnosis is clinical. However, an x-ray is often done to rule out damage to the joint.
Most of the cases of the bunion are treated by conservative means.
Acute symptoms can be treated with rest, ice and medication.
If the condition is asymptomatic, it might be better to watch and wait. Footwear modification and symptomatic treatment by drugs can be part of a treatment strategy.
Footwear Change
Better fitting shoes that fit properly do not compress the toes can lead to a decrease in the pain. These include shoes with wide toe box or using a stretcher for stretching the area that is tight.
Poorly-fitting shoes have been implicated in the development and worsening of the bunion.
Therefore, one should choose shoes carefully.
Select shoes with wide insteps, broad toes, and soft soles.
Avoid shoes that are too short, tight, or sharply pointed.
Heels should not be more than a few inches as higher heels put more pressure on the forefoot.
Padding
These are protective shields for the bunion. These pads cushion the painful area over the bunion. Sometimes the pain can worsen due to the pressure of the pad. Therefore, the product needs to be worn on a trial basis first.
Orthotics
Over-the-counter or custom-made orthotics could be shoe inserts or toe spacers.
Toe spacers can be placed between your toes.
Splints are to be worn and keep your toe in a straighter position may help relieve pain.
Medications
These include nonsteroidal anti-inflammatory medications and opioids.
Surgery
There are several surgical procedures to correct this condition.
Surgery is required to correct the deformity. there are many procedures described for this problem which work on the common treatment goal
- Removing the abnormal bony enlargement of the first metatarsal
- Realigning the first metatarsal bone relative to the adjacent metatarsal bone
- Straightening the great toe relative to the first metatarsal and adjacent toes
The age, health, lifestyle, and activity level of the patient may also play a role in the choice of procedure.
Newer, more stable procedures and better forms of fixation allow early rehabilitation.
Surgery is not considered in adolescent bunion unless the extreme pain is present that does not improve with a change in footwear or orthotic devices.
A multitude of procedures is available to correct the deformity, though the results of surgery can be quite variable if the deformity is not addressed directly. The procedures are briefly discussed in the next session.
Surgical Procedures for Hallux Valgus Correction
Distal Soft-Tissue Reconstruction
A mild deformity can be corrected with a distal soft tissue reconstruction which involves excision of medial eminence and capsule repair on the medial side along with the release of deforming structures on the lateral side.
This surgery requires that metatarsal head is not deformed.
This soft-tissue procedure is considered in
- Mild to moderate bunion deformity
- Hallux valgus angle less than 35 degrees
- The intermetatarsal angle is less than 15 degrees
- Distal metatarsal articular angle is not increased
Corrective Osteotomies
Corrective osteotomies can be done in phalanx or metatarsal depending on the locus of pathology.
Akin Osteotomy
It is the osteotomy of the proximal phalanx. It is often combined with medial eminence [bunion] excision and medial capsule repair.
This procedure is best for deformity in the proximal phalanx, also called Hallux Valgus interphalangeus [abnormal proximal phalanx articular angle].
The osteotomy can be done in conjunction with metatarsal osteotomy.
First-Metatarsal Osteotomy
First metatarsal osteotomy could be in the distal or proximal part of the metatarsal
Distal osteotomies are mainly for individuals with mild deformities.
- Allux valgus angle less than 30 degrees
- Intermetatarsal angle less than 13 degrees
- Distal metatarsal articular angle less than 15 degrees
Chevron osteotomy is a commonly done distal osteotomy and is considered quite reliable.
Proximal metatarsal osteotomies arey is considered for larger deformities, generally those with an intermetatarsal angle of greater than 15 degrees.
The osteotomies can be
- Medial opening-wedge osteotomy
- Lateral closing-wedge osteotomy
- Proximal chevron osteotomy
- Crescentic osteotomy
Arthrodesis and Resection
- First-tarsometatarsal fusion
- For moderate to severe osteotomies
- Hallux HVA greater than 30 degrees
- Intermetatarsal angle more than 15 degrees
- Hypermobile first ray
- Metatarsophalangeal joint subluxation
- Excisional arthroplasty (Keller)
- Rarely used
- Only in the elderly in low demand patients
- For moderate deformity with arthrosis
Complications of Surgical Procedures
Recurrence is a common across all the procedures but occurs more with just soft tissue procedures.
Closed wedge osteotomies may shorten the ray.
Metatarsalgia may occur from the loss of weightbearing function of the great toe.
Undercorrection and overcorrection are other known issues.