Last Updated on May 3, 2022
Cast syndrome is also known as superior mesenteric artery syndrome. It is an uncommon complication in the treatment of orthopedic conditions. It results from obstruction of the third portion of the duodenum due to the narrowing of the angle between the abdominal aorta and superior mesenteric artery.
Other names for cast syndrome are
- Wilkie’s syndrome
- Duodenal ileus
This was first described by Von Rokitansky in 1842 and later by Wilkie.
It is a rare syndrome and is more common in young females.
Mortality is around 33%.
It should be kept in mind that this obstruction can occur in absence of plaster also because there are many causes to mesenteric artery obstruction.
Cause of Cast Syndrome
 Most cases involve young adults.
Most cases involve young adults.
More than half of these cases have patients with scoliosis or kyphosis or treatment of hip conditions.
It has been seen after casting with
- Body jackets
- Shoulder spicas
- Hip spicas
Thus the common denominator is extensive coverage of the abdomen and chest.
Relevant Anatomy
The problem usually is located at the junction of the third and fourth parts of the duodenum, where the duodenum is bound by the ligament of Treitz. The duodenum passes across the anterior aspect of the lumbar spine from right to left at the level of the first and second lumbar vertebrae. Just above this point, the superior mesenteric artery arises from the abdominal aorta and passes downward with its accompanying veins in the mesentery.
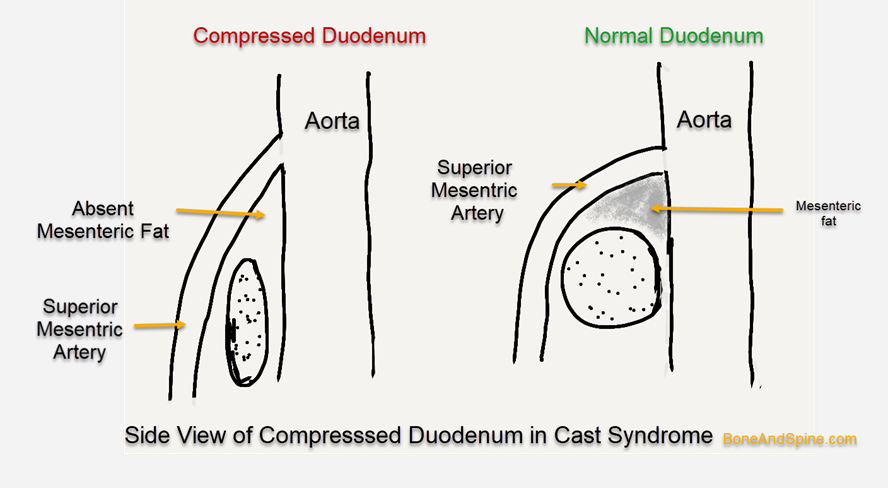 There is the potential for compression of the third portion of the duodenum between lumbar spine and aorta posteriorly and the mesentery and vessels anteriorly.
There is the potential for compression of the third portion of the duodenum between lumbar spine and aorta posteriorly and the mesentery and vessels anteriorly.
Two contributing factors are
- Recumbency or lying down- causes the weight of the mesentery to lie against the duodenum
- Increased lumbar lordosis, which tends to displace the duodenum anteriorly.
Gastric distention may aggravate the situation by forcing the remainder of the abdominal contents more distally and stretching the mesenteric vessels further leading to a spectrum of symptoms.
Clinical Presentation of Cast Syndrome
The signs and symptoms of cast syndrome are typical of upper intestinal obstruction.
They may develop insidiously or after several weeks after cast application or surgery.
The initial symptom is a feeling of fullness followed by nausea and vomiting.
Abdominal distention is obscured in the presence of a body jacket.
Following is the usual sequence of symptoms and signs
- Abdominal Distension
- Vomiting
- Intermittent in the early stages
- Becomes pernicious later
- Dehydration and metabolic alkalosis results
- Progressive metabolic derangement occurs
- Decrease in the passage of urine – oliguria, and shock may occur.
When these signs and symptoms occur in a patient who is in a body cast or who has had spinal trauma (including surgery), the diagnosis should be suspected.
Imaging
X-rays
X-rays of the abdomen may show early gastric dilatation. Contrast may help to reveal the distention of the stomach and the proximal portion of the duodenum. Usually, there is a sharp cutoff pattern at the region where the arteriomesenteric pedicle crosses the duodenum.
X-rays help to differentiate this syndrome from cholelithiasis, pancreatitis, gastric or duodenal ulcer, and high intestinal obstruction.
CT
CT abdomen with IV contrast helps to reveal the following
- Dilatation of stomach and proximal duodenum
- Decompression of rest of the duodenum and small bowel
- Aortomesenteric distance [normal 10-28 mm]
- Can be as low as 2 mm in cast syndrome
- Aortomesenteric angle
- Normal – 25–60 degrees
- Can be as low as 7 degrees in cast syndrome
Lab Tests
Most of the biochemistry blood works would come normal. In later stages electrolyte imbalance may occur.
Treatment of Cast Syndrome
- Removal of the offending plaster if any
- The absolute dietary restriction – Nothing by mouth
- Nasogastric tubing to conduct suction of the gastric secretions
- Intravenous fluids are essential to maintain hydration
- Correct any electrolyte or acid-base abnormalities
- Positioning the patient on the left side or prone relieves some of the effects of gravity in pulling the mesenteric pedicle against the duodenum. With the patient prone, tipping the bed to tilt the head down further decreases pressure from the pedicle.
- If these conservative measures are not sufficient to reverse the process, the treatment of choice is surgery duodenojejunostomy or gastrojejunostomy.
Prevention
Cast syndrome may be prevented by avoiding constrictive body casts that accentuate lumbar lordosis or prevent normal changes in abdominal contour. Patients at risk should be turned frequently or encouraged to move from side to side.