Last Updated on September 2, 2020
Congenital anomalies of shoulder are a group of disorders of the shoulder that affect shoulder anatomy and function.
Following congenital anomalies of shoulder are discussed in this article-
- Congenital dislocation of shoulder
- Congenital Glenoid Hypoplasia
- Aplasia of Scapula
- Torsional Deformity of Glenoid Cavity
- Congenital Varus Deformity of Proximal Humerus
- Torsional Deformity of Humeral Neck
Different Congenital Anomalies of Shoulder
Sprengel deformity
Sprengel deformity is a congenital condition where the scapula is small and located higher than its normal position because of its failure to descend to its position. There could also be scapular winging and presence of omovertebral bone 30-50%]. Omovertebral bone is an anomalous bone connecting the elevated scapula to the cervical spine. It is also called omovertebral bar and connects the superior medial angle of the scapula and cervical spine.
Sprengel deformity is also known by following names which refer to its higher position
- Congenital Elevation of the Scapula
- Congenital High Scapula
- Scapula Elevata
Sprengel deformity is the most common congenital malformation of the shoulder.
[Read more about Sprengel deformity.]
Congenital Dislocation of Shoulder
It is one of the congenital anomalies of the shoulder where the dislocation of shoulder present at birth.
It is of three types
- True congenital dislocation, developing in utero [Extremely rare]
- Dislocation caused directly by trauma at birth
- Acquired dislocation developing secondary to a brachial plexus injury. It is the most common type
In utero maldevelopment is the major cause for true congenital dislocations of the shoulder. This usually occurs due to bony abnormalities of the shoulder girdle.
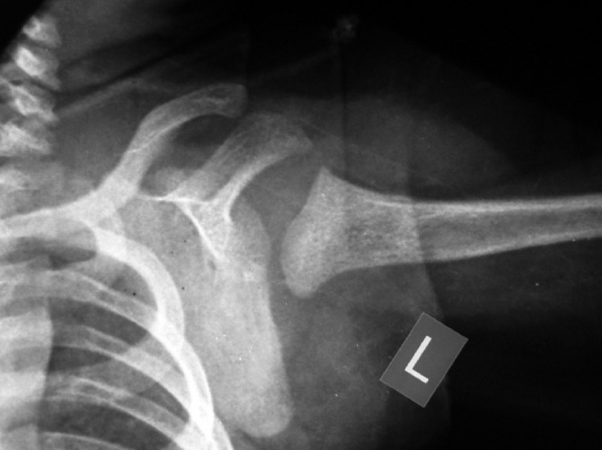
Image credit: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3100811/
The bony abnormality can be hypoplasia of the scapula or glenoid dysplasia.
X-rays can be used to detect and differentiate congenital dislocation of the shoulder from upper humeral fractures.
CT and MRI are much more sensitive in the diagnosis than radiographs and should be used when in doubt.
When functional impairment is minimal, no treatment is indicated. This is so because there is a possibility of further decreasing functional use of the limb.
Operative procedures employed depend on the individual case.
Where indicated, early reduction and containment of the humeral head in the glenoid socket might help achieve a satisfactory long-term outcome. Open reduction may be required for the release of contractures.
However, in severe malformations, surgical measures are often futile because the function cannot be improved.
Congenital Glenoid Hypoplasia
This malformation is due to incomplete ossification of the lower two-thirds of the cartilaginous glenoid and adjacent neck of the scapula because of failure of the formation of the lower and upper glenoid epiphysis. It is characterized in the radiogram by flattening, shallowness, and an underdeveloped appearance of the glenoid cavity.
The lower aspect of the clavicle may be hypertrophied into a bony prominence, and there may be spina bifida in the cervical region.
Often, the abnormality is bilateral and is encountered as an isolated malformation. It may be hereditary.
It was first described by Giongo and Heupke and is quite a rare condition.

Image credit: Hindawi
three groups of patients were identified
- Bilateral glenoid hypoplasia without instability of the shoulder
- bilateral glenoid hypoplasia with the instability of the shoulder
- unilateral glenoid hypoplasia and severe deformity of the humeral head
The cause and inheritance of glenoid hypoplasia are not well understood.
The scapula is ossified from following centers
- One for the body
- Two for the coracoid process
- Two for the acromion
- One for the vertebral border
- One for the inferior angle.
At birth, a large part of the scapula is osseous, but the acromion, coracoid process, glenoid, vertebral border, and inferior angle of the scapula are cartilaginous.
The glenoid fossa develops from a proximal and a distal center of ossification.
An aberration of one or both of these ossification centers has been implicated in the development of glenoid hypoplasia.
Following conditions have been noted to be associated with glenoid hypoplasia
- Erb’s palsy
- Muscular dystrophy
- Aseptic osteochondritis
- Hemophilic arthropathy
- Septic arthritis in newborn
Glenoid hypoplasia is often diagnosed as an incidental finding on x-ray as many patients are asymptomatic. The symptoms may appear in the second or third decade of life and include pain, restriction of motion, and instability.
X-rays reveal
- Shallow and irregular glenoid fossa
- Prominent coracoid process
- Large and elongated ribs
- Flattening of the humeral head.
Most cases have been managed by nonoperative measures which include symptomatic treatment and monitoring.
Glenoid osteotomy may be done to restore the normal version of the glenoid if recognized early.
In case of glenohumeral arthritis occurring in old age, total shoulder replacement may be an option.
Aplasia of Scapula
Congenital absence of the scapula is extremely rare. It is usually associated with ipsilateral Amelia. Treatment consists of fitting with an upper-limb prosthesis.
Torsional Deformity of Glenoid Cavity
This deformity will cause posterior or anterior dislocation of the shoulder and can be demonstrated on an axillary radiogram or a computed tomographic torsion study of the glenoid cavity.
Treatment consists of osteotomy of the neck of the scapula and insertion of a wedge bone graft to correct the abnormal glenoid torsion.
Congenital Varus Deformity of Proximal Humerus
This malformation may be developmental or secondary to neurofibromatosis or rachitic syndromes.
Torsional Deformity of Humeral Neck
Excessive retroversion will cause posterior dislocation of the glenohumeral joint, and excessive anteversion will cause anterior dislocation. Computed axial tomography will show the degree of humeral torsion. When torsion deformity is severe and is causing shoulder joint instability, it is treated by derotation osteotomy.