Last Updated on November 10, 2019
A corn is a thickening of the skin due to friction and pressure that is usually intermittently occurring.
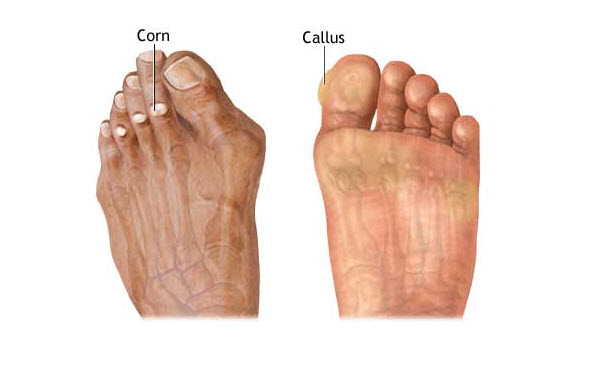
Clavus is a general term covering both corn and calluses [see the difference below]
The term implies the thickening results from hyperkeratosis and may result in chronic pain.
Clavi [plural of cavus] are common worldwide. The most common sites for corn occurrence are the feet. Corn occurs on toes and other parts of the feet where friction occurs
They are more common in women than in men.
Anyone can have a clavus, but most individuals acquire the risk factors for clavus formation after puberty.
Recurrence is common.
Definitions
Clavus or corn or callus is known by many names. It is important to understand the subtle differences among the common usage through the term clavus covers everything.
Callosity or calluses develop from forces distributed over a broad area of skin whereas corns develop from more localized forces. Corns can occur within an area of callus, such as on the plantar surface.
Corn
A corn is a circumscribed, sharply demarcated area of traumatic hyperkeratosis with a visible translucent central core which presses deeply into the dermis, causing pain and sometimes inflammation.
Corn is also known by name of heloma. It is of following types
Hard Corn
Also called heloma durum, a dry horny mass. It is most commonly found on the dorsolateral aspect of the fifth toe or the dorsum of the interphalangeal joints of the lesser toes. It is termed as the digital corn.
Soft Corn
The soft corn or heloma molle is a painful lesion that occurs interdigitally. It is also called interdigital corn.
Periungual Corn
The third type is a periungual corn, and this type occurs near or on the edge of a nail.
A plantar corn is a type of hard corn most commonly associated with a central core. Plantar corns that do not respond to conservative medical treatment are referred to as intractable plantar keratosis.
Callus/ Callosity
A callus occurs when the process of keratinization of the epithelium becomes overactive due to shearing or compressive forces.
A callus is usually larger, does not have a central core [than corn], and may or may not be painful. Calluses often form as normal protective response as seen in the hands of manual laborers and the feet of those who walk barefoot. A callus or callosity is pathological only when it causes symptoms.
For all practical purposes, callosity and callus are same.
Risk Factors for Corns
Corns are often seen in athletes and in patient populations exposed to uneven friction from footwear or gait abnormalities which include
- Abnormal foot mechanics
- High activity level
- Peripheral neuropathy
- Bony prominences
- Prominent condylar projection
- Malunion of a fracture
- Faulty foot mechanics
- Cavovarus foot
- Toe deformity (claw, hammer, mallet)
- Short first metatarsal
- Hallux rigidus
- Osteotomy or removal of the adjacent metatarsal head
Conditions associated with clavus formation include the following:
- Advanced patient age
- Amputation ( stump callosities)
- Doxorubicin toxicity
- Keratoderma palmaris et plantaris
- Obesity
- Pachyonychia congenita
- Sensory neuropathies, including neuroborreliosis
- Tethered spinal cord syndrome
- Vascular occlusion syndromes
- Warts
- Rheumatoid arthritis
- Diabetes mellitus with associated peripheral neuropathy
- Obsessive-compulsive disorder (pseudo-knuckle pads)
- Ectopic nail
Pathophysiology
Corns are the result of mechanical trauma to the skin culminating in hyperplasia of the epidermis. The foot is the most common
Bones of the foot have many projections, especially over the condyles of the heads and bases of the metatarsals and phalanges. Pressure by a tight shoe during walking irritates the skin and body attempts to protect by the accumulation of the horny layer [stratum corneum] of the epithelium. v But this thickening itself causes a prominence that increases the pressure in a tight shoe, thus creating a vicious cycle that may ultimately lead to the keratin plug pressing into the dermis and causing pain.
Abnormal mechanical stresses may be extrinsic (from without) or intrinsic (from within).
As corn formation ensues, friction against the footwear is likely to perpetuate hyperkeratosis.
With corns, external mechanical forces are focused on a localized area of the skin and formation of a hard keratin plug that presses painfully into the papillary dermis [radix or nucleus]
Deformities like toe deformity, including contractures and claw, hammer, and mallet-shaped toes, or deformities from pathologies like rheumatoid arthritis can contribute to clavus formation
The long-term or repetitive motion may also induce clavus formation, as is seen in computer users and text messengers (ie, “mousing” callus.
People who sit for prolonged periods in crosslegged position are known to have callosities on bearing surfaces of the ankle.
Clinical Presentation
Commonly, a patient reports the development of a localized growth on their foot or toes. these corns on toes or corns on feet cause pain on walking or when wearing shoes.
Clinically, all variants of clavus lesions look like hyperkeratotic or thick skin. Maceration and secondary fungal or bacterial infections are a common overlying feature in heloma molle and diabetes. Plantar helomas or corns tend to have a central keratin plug having a clear, firm, central core.
Gait should be observed to identify irregular mechanics. It is important to differentiate corns from warts as they could present in the same manner.
- Direct pressure causes tenderness in corn whereas warts are tender with pressure applied from side to side.
- Plantar warts do not have a central core.
- There is no capillary dotting on paring hard corns as compared to plantar warts
A soft corn is boggy and macerated so that it appears white. Soft corns usually occur in the fourth interdigital space.
Examination of patients should include an assessment of the types of footwear worn, activities performed, gait, and current home therapy or previously prescribed therapy.
Lesions should be palpated and pared to look for underlying blood vessels (black dots or pinpoint bleeding), which are seen in warts, and to look for underlying ulcerations, as seen in neurovascular ulcerations (especially in patients with diabetes).
Pedobarographic studies are pressure assessments that may be used to detect an altered distribution of foot pressure. MRI may delineate diabetic foot problems more clearly.
Biopsy of lesions reveals hyperkeratosis and, occasionally, mucin deposition.
Treatment of Corns
Paring
Pairing refers to sequential slicing to reduce the lesion size.
Pairing of the lesions immediately reduces pain. It can be done or without anesthesia until the central keratin core is removed.
Pressure or Friction removal
This calls for an accurate determination of the cause so that causation if possible can be eliminated. This includes better footwear, the use of orthotics like toe spacers to remove pressure etc.
For example, shoes with extra length for toe deformity, and shoes with extra width are required for lateral toe callosities help to ease out the pressure.
Switching to soft shoes without seams would reduce the friction.
Similarly, reduction of heel height may be helpful for patients with metacarpal head callosities.
Foot orthotics can help with foot dynamics.
Patients are advised to reduce or eliminate certain mechanical forces or motions.
Keratolytic Agents
Keratolytic agents remove the keratin layer, a form of chemical debridement. Following agents are commonly used.
- 40% salicylic acid pads and plaster
- 40% urea cream
- 12% lactic acid cream.
Combination products are also available.
These can be used as self-adhesive pads, lotions, creams, and medicaments.
Filler Injections
It involves Injection of 0.1 mL of medical-grade liquid silicone below a clavus and above the bone
Laser
A carbon dioxide laser can be used to pare deep lesions.
Intralesional Injections
Intralesional triamcinolone and topical vitamin A acid compounds also may reduce localized hyperkeratosis.
Other Treatments
Soft Corns
- Properly fitting footwear
- Better foot hygiene
- Antifungal or antibacterial powder after washing the area
- Toe spacer are additional techniques used to treat soft corns. [
Plantar Callosities
Vacuum orthoses for diabetic patients with plantar callosities.
Surgery
Surgery to remove the bony prominences is indicated only if all conservative measures fail
- Bunionectomy
- Syndactylization – Excision of the apposing skin surfaces between the fourth and fifth toes
- Osteotomy
- Arthroplasty
Chronic foot pain despite conservative therapy is the primary indication for surgery.
Hallux valgus correction may aid in the reduction of painful callosities over the long term.
Surgical corrections for claw, hammer, and mallet toes are simple procedures.
Shaving of prominent condyles of bony prominences may be beneficial, particularly on the fifth digit.
Arthroplasty of the fifth toe interphalangeal joint also may be performed.
For metatarsal head pressure, metatarsal condylectomy or chevron osteotomy may be performed to relieve metatarsal head pressure.
Complications of Corn
- Secondary bacterial or fungal infection
- Septic arthritis or osteomyelitis [when near the joint]
- Ulcerations from chronic pressure [esp in diabetics]
- Maceration
References
- Freeman DB. Corns and calluses resulting from mechanical hyperkeratosis. Am Fam Physician. 2002 Jun 1. 65(11):2277-80.
- Farndon L, Concannon M, Stephenson J. A survey to investigate the association of pain, foot disability and quality of life with corns. J Foot Ankle Res. 2015. 8:70.
- Singh D, Bentley G, Trevino SG. Callosities, corns, and calluses. BMJ. 1996 Jun 1. 312(7043):1403-6
- Coughlin MJ, Kennedy MP. Operative repair of fourth and fifth toe corns. Foot Ankle Int. 2003 Feb. 24(2):147-57.
- Bevans JS, Bosson G. A comparison of electrosurgery and sharp debridement in the treatment of chronic neurovascular, neurofibrous and hard corns. A pragmatic randomised controlled trial. Foot (Edinb). 2010 Mar. 20(1):12-7.
- Balkin SW. Injectable silicone and the foot: a 41-year clinical and histologic history. Dermatol Surg. 2005 Nov. 31(11 Pt 2):1555-9; discussion 1560.
- Brousseau-Foley M, Cantin V. Digital and interdigital corns: a report of two cases with use of hyaluronic acid gel filler. J Am Podiatr Med Assoc. 2014 Jul. 104(4):413-6.