Last Updated on April 23, 2022
Acute elbow dislocation in adults occurs at the ulnohumeral joint. Elbow dislocation can be pure dislocation or associated with fractures of surrounding bones.
Elbow is a very important part of upper limb function and plays a very important role in the positioning of the hand for grip and prehension. Various day to activities and recreational and sports activities require a wide range of movement at the elbow in both flexion and extension and forearm rotation.
Elbow is relatively a stable joint and is dislocated by sufficient force. Because of their vicinity, the neurovascular bundle is quite vulnerable to injury in an elbow dislocation.
The elbow dislocation accounts for 10-25% of injuries to the elbow. The posterolateral elbow dislocation is the most common type of dislocation accounting for as much as 80 percent of dislocations.
Sports injuries account for 50 percent of elbow dislocations.Adolescents and young adults constitute the majority

Relevant Anatomy
[Read detailed anatomy of elbow]
The elbow is primarily a hinge joint for flexion-extension. But it also allows for pronation and supination.
Ulnohumeral joint is formed by the humerus and the ulna is the main elbow joint. It is a very stable joint due to its peculiar bony anatomy and a considerable force is necessary to dislocate the elbow.
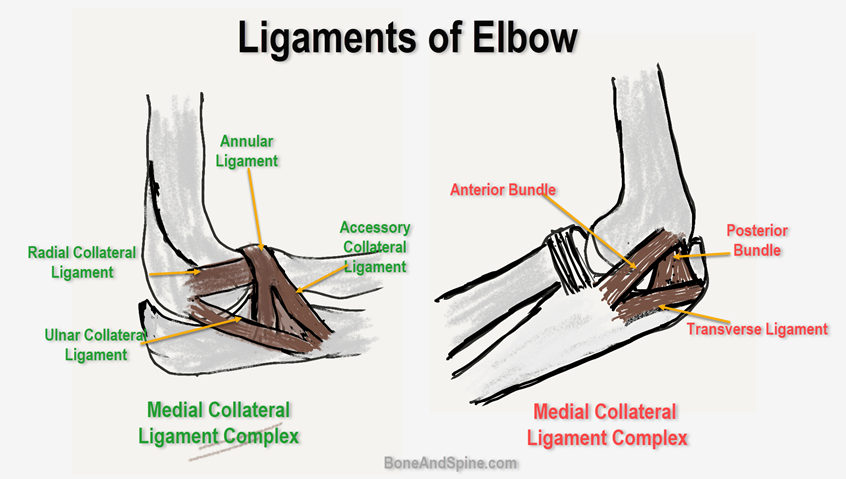
The medial collateral ligament and lateral collateral ligament add to the elbow’s natural bony stability.
The medial collateral ligament consists of 3 bands
• Anterior oblique
• Posterior oblique
• Transverse
• The anterior band provides most of the resistance to valgus stress
The lateral collateral ligament has 2 bands, the ulnar collateral and radial collateral.
Proximity of brachial artery, median nerve and ulnar nerve to the joint makes them vulnerable to the injury.
The dislocations generally begin with teraing of lateral collateral ligament and then moves to anterior and posterior compartments. Medial collateral ligament is finally damaged with continued force.
Classification of Elbow Dislocation
Most of the classifications refer to the position of the ulna relative to the humerus after injury. For example, a posterior dislocation refers to the ulna and radius sitting posterior to the humerus.
Injury can be classified as
- Posterior
- Posteromedial
- Posterolateral
- Anterior
- Medial
- Lateral
- Divergent
Most acute elbow dislocations are posterior. Anterior, medial, lateral, and divergent forms are very rare.
Mechanism of Injury
Posterior dislocations of the elbow are commonly caused by a fall on the hand or wrist.
Therefore, sports that increase the likelihood of a person falling onto an outstretched hand like gymnastics, rollerblading, and cycling may increase the risk of elbow dislocation.
During the fall, as force is transmitted to the extended elbow, a resultant anterior force levers the ulna out of the trochlea. As the joint continues to hyperextend, the anterior capsule and collateral ligaments are placed under increasing tension and eventually fail.
Anterior dislocation may be caused by an impact on the posterior forearm in a slightly flexed position.
Clinical Presentation of Dislocated Elbow
The patient would present with a history of fall on the hand or wrist. There would be a history of elbow giving way after that following which the patient was unable to use his elbow. There would be extreme pain in the elbow and the patient generally supports the elbow to av0id any movement.

On examination, there would be deformity and swelling of the elbow with change in epicondylar and olecranon relation. The triceps tendon may appear taut.
The limb should be examined for arterial and brachia injuries. A detailed examination of the brachial artery, median and ulnar nerves should be carried out.
Imaging
Anteroposterior and lateral views of the elbow are sufficient for diagnosis. X-rays also allow an analysis of associated fractures if any.
Often the dislocations are quite obvious. But sometimes, a subluxation can be difficult to identify. A line drawn through the center of the radial neck should intersect the center of the capitellum in any view of the elbow.
CT is useful in assessing associated fractures, especially the coronoid process fractures.
In case of an arterial injury, color doppler and arteriography help to find the injury and plan the treatment.
Treatment of Elbow Dislocation
An uncomplicated pure dislocation of the elbow can be easily treated by closed methods. In the case of associated fractures, the treatment varies according to the fracture pattern.
In case of vascular injury, the repair of the vessel is the first priority. However, in associated nerve injuries, the treatment of closed reduction and plaster application can be very well initiated and observed.
If the dislocation is open with a large wound over the elbow, surgery is almost always required.
Nonoperative Treatment
This involves closed reduction of the elbow and immobilization with a splint in more than 90 degrees of flexion for about two weeks.
[Read- What is a splint?]
Before applying splintage, it must be ensured that ulnohumeral and radiocapitellar joints are concentrically reduced.
The presence of minor undisplaced fractures is not a contraindication to closed treatment
After mobilization, progressive range of motion exercises are started. Extension splints may be needed the night.
Operative Treatment
Operative treatment is required in case of irreducible dislocations and associated fractures. The indications for surgery are
- Terrible triad elbow injury [Radial head fracture, a type III coronoid fracture, and an associated elbow dislocation]
- Coronoid fractures involving more than 10% of the coronoid
- Persistent instability of the elbow after reduction and fixation [requires MCL repair]
- Arterial Injury that needs reconstruction
The choice of surgery depends on the associated fractures and may vary from K-wire to radial head replacement.
Elbow dislocation with confirmed arterial injury is an emergency surgery because of arterial reconstruction.
So if the pulse at the wrist does not return after the reduction, the patient should be investigated for arterial injury and once the lesion has been identified, the patient should be prepared for immediate arterial reconstruction.
For elbow dislocations with a nerve injury that does not improve after the reduction, it is best to wait and watch for recovery. If no sign of recovery is noted till 3 months, an operation should be considered.
In case of open injury, early exploration should be done.
In case the injury to the nerve occurs at the time of the reduction, exploration is indicated.
Special Scenarios in Elbow Dislocation
Anterior Elbow Dislocation

Anterior dislocation of the elbow is quite rare.
It usually occurs after a fall which results in a force striking the posterior forearm in the flexed position.
Because of the mechanism of injury, a fracture of the olecranon commonly occurs with this injury.
Because the dislocation is anterior, injury to nerves and vessels can occur frequently.
The reduction maneuver is the reverse of the posterior dislocation.
Medial and Lateral Elbow Dislocation

Medial and lateral dislocations present with a widening of the elbow.
The diagnosis should be suspected if the mediolateral widening of the elbow is present.
In the anteroposterior x-ray, a pure medial or lateral dislocation shows the greater sigmoid notch of the ulna in the plane of the distal humerus
Divergent of the Elbow Dislocation
Divergent dislocation of the elbow is another rare type of dislocation. In this, the radius and ulna dislocate in diverging directions.

The divergent injury causes substantial soft tissue trauma.
Image Gallery of Elbow Dislocation









References
- O’Driscoll SW. E5. Parsons BO, Ramsey ML. Acute elbow dislocations in athletes. Clin Sports Med. 2010 Oct. 29(4):599-609.
- Sheps DM, Hildebrand KA, Boorman RS. Simple dislocations of the elbow: evaluation and treatment. Hand Clin. 2004 Nov. 20(4):389-404. [ Link].
- Micic I, Kim SY, Park IH, Kim PT, Jeon IH. Surgical management of unstable elbow dislocation without intra-articular fracture. Int Orthop. 2009 Aug. 33 (4):1141-7.
- Englert C, Zellner J, Koller M, Nerlich M, Lenich A. Elbow dislocations: a review ranging from soft tissue injuries to complex elbow fracture-dislocations. Adv Orthop. 2013. 2013:951397.