Last Updated on October 29, 2023
Fibula fracture occurs less commonly in isolation and more commonly occur in association with a tibia fracture. Therefore, if a displaced fibula fracture is encountered, fracture of tibia bone must be suspected and looked for.
At either end of the bone, the fracture may also occur with ligament injuries.
The fibula and tibia are the two long bones of the lower leg. Joined together at knee and ankle joints.
The fibula is the smaller bone of the two.
The fibula bone is expendable for most of its part except in distal third of the leg where it forms an important part of ankle joint. That means it can be used for purpose of strut grafting without compromising the limb function.
Anatomy of Fibula Bone
The fibula bone is comparable to the ulna bone of the upper limb and is considered homologous to each other. The fibula is a located on the lateral side of the tibia and connected with it at upper and lower end.
The tibia is called shin bone whereas fibula is called calf bone.
The fibula has an upper end, shaft, and a lower end.
The upper end is slightly expanded in all directions and articulates with the corresponding surface on the lateral condyle of the tibia. The constricted part further down is called neck of the fibula and is important because common peroneal nerve curves round it and can get injured because of fracture in this region.
The shaft of the fibula is thin and shows considerable variation in its form as the muscle force of attached muscles determines the shape.
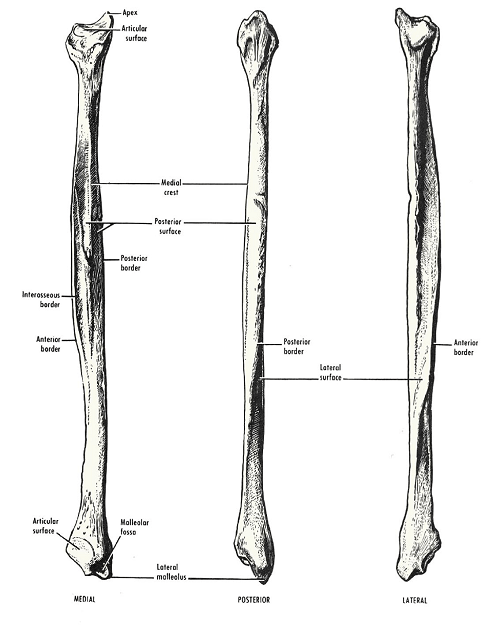
It is also called lateral malleolus and along with the inferior surface of the tibia and medial malleolus participates information of ankle joint.
The tip of the lateral malleolus is 0.5 cm lower than that of the medial malleolus, and its anterior surface is 1.5 cm posterior to that of the medial malleolus. It has the following four surfaces.
Know more about the anatomy of fibula.

Causes and Types of Fibula Fracture
Most of the fractures of fibula occur in association with fractures of the tibia. Isolated fibula fractures are seen in the lower end of fibula [Often there could be a ligament injury present.]
Most of the fractures of the fibula are the result of trauma.
In ankle injuries, fibula fracture is also seen with ligamentous injuries.
Tibial fractures are often high energy injuries and often the force of fracture breaks fibula too.
Stress fractures of fibula may occur due to repetitive loading.
Lower end fibula fractures are common in older adults.
In older adults, decreased bone mass is a risk factor for fractures and fractures of fibula are no exception. Distal end fibula fractures are common in such situations.
Most studies show that females have the highest number of fibular fractures among older adults through some studies have challenged this.
Cigarette smoking is an important risk factor.
Athletes involved in contact sports have a higher incidence of fibular fractures. Football and rugby are typical examples, downhill winter sports like snowboarding and skiing.
It is interesting to note that skiers often fracture the proximal third of the tibia-fibulae whereas snowboarders often have fractures of the distal third of the fibula.
Isolated fibula fracture may occur due to forceful landing after a high jump or direct injury on the outer aspect of the leg.
Depending on the region involved the fibula fractures may occur in the proximal fibula, the shaft of the fibula and distal fibula.
Fractures of Proximal Fibula
- Avulsion Fractures
- Fibular head fractures
Fractures of Shaft of Fibula
- Often caused by a direct blow
- Stress fractures
Distal Fibula Fractures
- Lateral malleolus fractures
- Avulsion fractures of the lower fibula
Clinical Presentation of Fibula Fracture
After an injury, pain, swelling, and tenderness would be present in the region of injury. The fracture could be in the upper end, shaft or lower end of the fibula.
In most of the cases, especially with associated tibial fractures, the patient would not be able to bear the weight due. When there is an isolated fracture of the fibular shaft or an undisplaced lateral malleolus fracture, painful weight bearing is possible.
Numbness of the feet or motor weakness may be present especially in the fractures near the fibular neck. A fracture in this region may cause injury to common peroneal nerve and result in the neural deficit.
Knee effusion and ankle effusion may be seen in proximal fractures which are often associated with tibial plateau fractures or ligament injuries.
Imaging
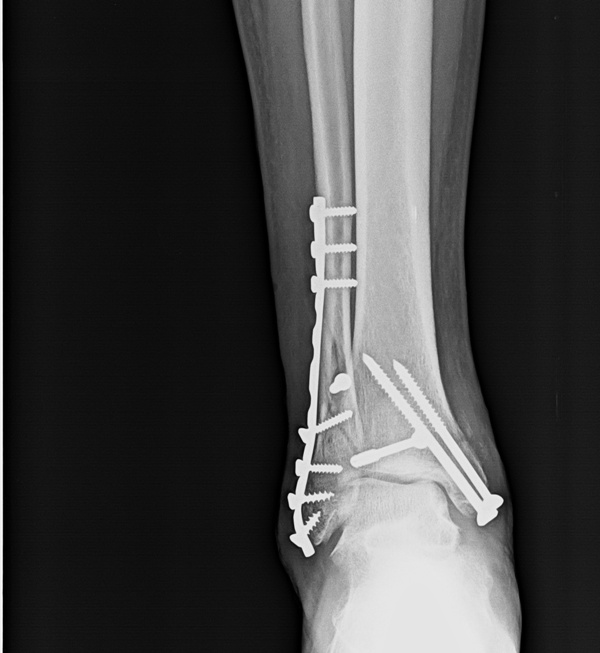
X-ray is the basic and in most cases the only investigation required. Anteroposterior and lateral views are generally sufficient for fractures of the fibula. But if the joint on either side is involved, additional investigations may be needed to study joint injuries [not fibula per se]
X-rays reveal a fracture site, fracture pattern and any associated injuries. In lower fibula fractures, the ankle joint should be looked for any widening of the joint space which indicates subluxation.
In cases of the stress fractures or pathological fractures, further studies like MRI or bone scan may be required.
Treatment of fibula Fracture
Fractures of the Proximal fibula and Fibular Shaft
The treatment of the fibula fractures depends on the region of the fibula broken, whether associated fracture of the tibia is present or not and whether the fracture is open.
Except for displaced fractures of lateral malleolus [lower fibula], the fracture of the fibula is not a main consideration of the treatment of the injury. The treatment is mainly guided by the condition of the other bone – the tibia.
Therefore, in proximal fractures and fractures of the shaft of fibula, fractures of the tibia is that is considered for treatment. The fibula is often not given importance.
The fracture of the tibia may be treated in a cast or undergo surgery.
When a cast is a treatment, the fibula is also treated along in the cast.
If the tibia is treated by surgery, the fibula is not operated in most of the cases as its union is not of consequence.
For example in the interlocking of the tibia, the fibula is not touched.
In most of the cases, however, anatomical reduction of tibia brings fibula in enough alignment so that it unites. But even if it does not, it is accepted.
Lately few authors have advocated plating of the shaft of fibula along with tibial surgery to provide added stability but there is no consensus on it yet.
As usual, open fractures are surgical emergencies and need debridement and suitable fixation. But again this needs to be explained.
Open fractures of the tibia are the definite surgical emergency requiring debridement and fixation.
But a closed fracture tibia and open fracture fibula is not at par with the previous injury. Debridement is necessary but fixation is done only if tibia requires.
In case, the open fracture is treated in a cast, a window is opened in the cast for wound examination and dressing.
Fractures of Distal Fibula
In contrast to fractures of proximal fractures and fibular shaft fractures, fractures of the distal third of fibula assume importance and even guide the treatment.
This is because the distalmost fibula participates in the ankle joint and any fracture within 7-10 cms of the joint line affects the stability of the ankle joint.
If within that region, fibula needs to be anatomically reduced and fixed when displaced. Displacements often causes the ankle joint to be subluxed [evident by widening of joint space]
If the fracture is isolated and undisplaced, and the ankle joint is not subluxated, the patient just needs immobilization.

Follow Up
In upper fibula and shaft fractures, the postoperative protocol is determined by the injury and treatment of the other bone. For example, the patient is kept nonweight bearing in upper tibial fractures.
However, in the case of interlocking for the shaft of the tibia, immediate weight bearing is allowed.
Distal fibula fracture needs to remain nonweight bearing until the fracture has united both with surgical or conservative treatment.
The patient is put on physical therapy at an appropriate time during the course of treatment
Fibula fracture often heals without an issue. Rarely, nonunion may occur which is not of consequence except when it is in the lower third of the bone.
Compartment syndrome or common peroneal nerve injury may lead to their own complications if they occur.