Last Updated on April 29, 2022
Forearm fractures are very common in young active adults. These fractures generally include at least one or both of the forearm bones namely radius or ulna.
Fractures of proximal and distal portions of these bones are special fractures and are discussed separately.
This article addresses the injury to the diaphyseal radius and ulna without an associated distal or proximal radioulnar joints injury. These injuries are discussed separately and links are given below
On most occasions, both bones fracture together. In the case of single bone fractures, the proximal or distal joint might be injured.
Radisu and ulna fractures demand meticulous fracture reduction as shortening and angulation of the forearm bones can cause many functional problems.
Therefore, precise reduction for anatomical restoration and secure fixation is very necessary in forearm fractures.
Relevant Anatomy of Forearm Bones
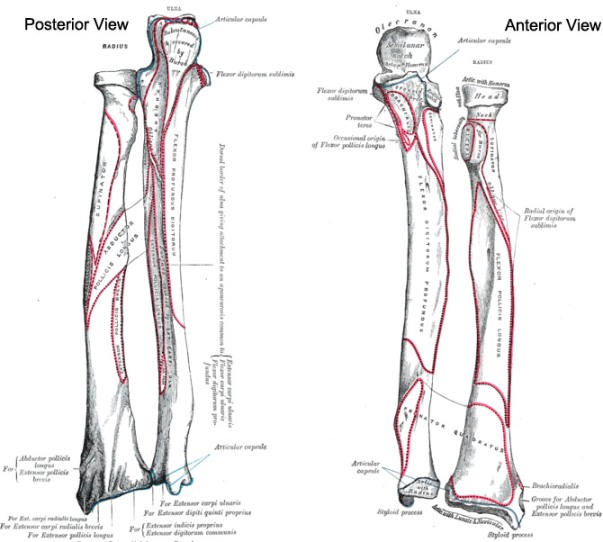
The radius and ulna are two bones of the forearm and connect at the proximal and distal radioulnar joint at either end.
Ulna bone is relatively straight bone. It articulates with the distal humerus at the elbow and runs virtually subcutaneously distally to the ulnar styloid at the wrist.
The other bone, the radius is bowed. Its articulation with capitellum of humerus angles at least 13° opposite to the bow.
The distal radioulnar joint is such that it allows the radius to sweep around the relatively fixed ulna with pronation and supination.
The space between the two bones is traversed by the interosseous membrane that runs obliquely. It originates at proximal radius and inserts at distal radius.
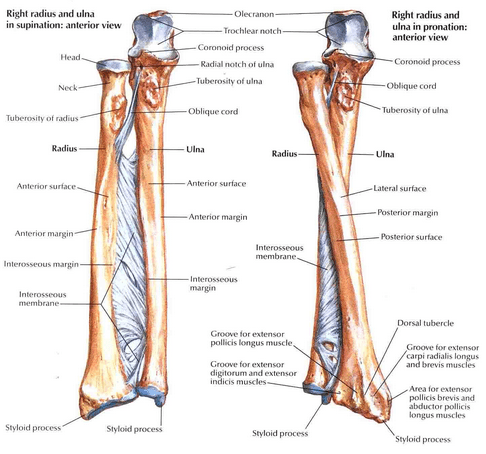
Radial bow and interosseous space must be preserved for normal motion of the forearm.
Mechanism of Injury of Forearm Fractures
Forearm fracture can be caused by various mechanisms. The most common is motor vehicle injury especially automobile and motorbike injuries. Most of these vehicular accidents result in some type of direct blow to the forearm.
Direct trauma by an object such as a stick etc also can cause the fracture of these bones.

Gunshot wounds can cause forearm fracture. Such injuries are commonly associated with nerve or soft tissue deficits and frequently have a significant bone loss.

Another cause is pathological forearm fracture and in such cases, a previous underlying pathology is responsible for the injury. This injury can result from trivial trauma, a force that normally would not cause a break in the normal bone.
Forearm fractures can occur as a result of falls.

Clinical Presentation of Forearm Fractures
In adults, it is very rare for these fractures to be undisplaced. As radius and ulna are strong bones, an injury of sufficient force is required to break them which would cause displacement.

The patient of fractured radius and ulna will have a history of significant trauma and symptoms include
- Pain
- Swelling
- Deformity
- loss of associated function of the forearm.
The presence of a wound is likely to make the fracture open. Therefore any wound, especially near the fracture site, should be examined for communication with fracture hematoma. A careful neurologic evaluation of the motor and sensory functions of the radial, median, and ulnar nerves should be done. Amount Distal pulses should be palpated to check for the vascular status of the forearm.
Swelling of the forearm should be assessed to rule out compartment syndrome. A simple clinical test to diagnose compartment syndrome is a passive stretch of the fingers. If the pain in the forearm is present when the fingers are passively extended, compartment syndrome is probably present.
If the patient is noncooperative or unconscious, compartment pressures should be measured to rule out the possibility of compartment syndrome.
Imaging
A simple anteroposterior and lateral radiograph of the forearm would help to diagnose the fracture pattern and the level of forearm fracture. Wrist and elbow joints should be included in the radiographs to rule out any associated injury.


The configuration of midshaft fractures of the radius and ulna varies depending on the mechanism of injury and the degree of violence involved.

Low-energy fractures tend to be transverse or short oblique, whereas high-energy injuries are comminuted or segmented and are often associated with extensive soft tissue injuries.
Comminuted fractures are generally as a result of direct trauma to the bone.


A line drawn through the radial shaft, neck, and head should pass through the center of the capitellum on any radiographic view of the elbow. This simple test can determine any associated elbow injury.
In case of doubtful wrist and elbow injuries computed axial tomography can be undertaken to look for subtle injuries. It is better to involve the normal part of the opposite limb for comparison.

Treatment of Forearm Fractures
Goals of forearm fracture treatment are
- Anatomic reduction
- Rigid fixation,
- Early mobilization
The majority of displaced fractures of the shafts of the radius and ulna are treated by the operative method. Closed treatment of forearm fracture should be undertaken only if there is a specific contraindication to operative treatment.
Cast Immobilization
Simple cast immobilization is used in undisplaced fracture of both bones of the forearm in adults. However, this entity is very rare in adults.

Following cast application, x-rays should be done at weekly intervals. It is very common for these fractures to become displaced later, therefore they should be watched. In case the displacement occurs, it should be treated as a displaced fracture.
Operative Treatment
Displaced fractures of forearm do not yield satisfactory results with closed treatment and should be operated whenever possible.
Operative treatment allows for accurate fracture reduction and secure fixation.

To achieve excellent results, anatomical reduction and stable fixation are required. Restoration of normal bone length will prevent subluxation of either the proximal or distal radioulnar joint and will reestablish length to the muscles. Restoration of rotational alignment is essential for normal pronation–supination function of the forearm.

Open reduction and Internal Fixation using plate fixation is the standard treatment for closed, displaced fractures of the forearm. These fractures of both bones of the adult should be fixed as soon as feasible preferably within the first 24 to 48 hours of injury because the fractures lying in liquid hematoma are easier to reduce and fix.

But these fractures should be fixed any time irrespective of the delay for whatsoever reason.
Stainless steel, limited-contact, the dynamic compression plate is the treatment of choice for displaced fractures of the radius and ulna and provide very good results.
The preferred plate is the eight-hole dynamic compression plate with 3.5-mm cortical screws.
Though plate and screw combination takes care of most of the fracture configurations, there are some situations like open fractures, segmental fractures, failed plating and multiple injuries where nailing might be preferred.
The disadvantage of the plating is extensive soft tissue dissection and periosteal stripping. The advantage is the ability of the surgeon to reduce and fix fractures in anatomical position.
Fixation with intramedullary nails is not preferred as the nail is a poor implant as compared to plate in the context of forearm. It is not able to control rotation and cannot maintain a radial bow.
It should be reserved for selected indications. The anatomical reduction is of paramount importance in these fractures and that is difficult to achieve with nails.
In the presence of multiple injuries, all the injuries should be fixed.
External fixators are used in case of open injuries or massive soft tissue loss[Gustillo IIB and above]
Open forearm fractures require emergency treatment. The treatment needs to be individualized depending upon patient profile and wound.
In case of bone loss, bone grafting may be considered.
Complications of Forearm Fracture
The complications associated with forearm fracture can be due to injury per se, failure to get the right treatment or complications of treatment as such. Many complications are general complications associated with any fracture and few are specific to these fractures.

Here is a list of most common complications of these fractures.
- Infection
- Injury to nerve and/or vessel
- Compartment Syndrome
- Posttraumatic Radioulnar Synostosis
- Soft tissue tethering
- Malunion/Nonunion
References
- Richard MJ, Wartinbee DA, Riboh J, Miller M, Leversedge FJ, Ruch DS. Analysis of the complications of palmar plating versus external fixation for fractures of the distal radius. J Hand Surg Am. 2011 Oct. 36 (10):1614-20. [Link].
- Droll KP, Perna P, Potter J, Harniman E, Schemitsch EH, McKee MD. Outcomes following plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am. 2007 Dec. 89 (12):2619-24. [abstract]