Last Updated on August 29, 2021
Galeazzi fracture-dislocations is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. The ulnar shaft is intact.
A fracture of distal radius Galeazzi-equivalent fracture is a distal radial fracture with a distal ulnar physeal fracture 2.
Most of these fractures are seen in children, with a peak incidence at age 9-12 years.
Adult Galeazzi fractures account for less than 7 percent of forearm fractures.
Typically, Galeazzi fracture-dislocations occur due to a fall on an outstretched hand (FOOSH) with the elbow in flexion leading to axial loading on the hyperpronated forearm
It is named after surgeon, Riccardo Galeazzi, who described this fracture in 1934 though Cooper was first to describe this injury pattern in 1842.
The incidence instability of radial fracture is 55% when the fracture is within 7.5 cm from the articular surface. When the radial fracture is more than 7.5 cm from the articular surface, this incidence is 6%.
Fractures in the proximal two-thirds of the radius are not associated with injury to the distal radioulnar joint.
Relevant Anatomy and Mechanism of Injury
The radius and ulna bones form the bony framework of the forearm. Three main stabilizers of this frame are triangular fibrocartilage distally, interoseous membrane which connects both the bone, and annular ligament which holds the proximal radius.
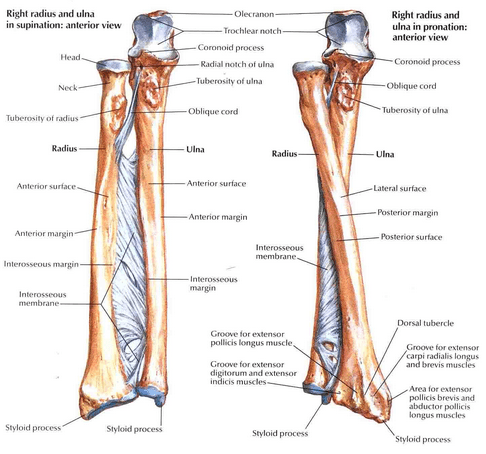
The ulnar head, distally, serves as an insertion point for the TFCC and supplements distal radioulnar joint.
Proximally, radial head articulates with the capitellum of the humerus to form radiocapitellar joint rotating within the annular ligament during pronation and supination.
Distal radioulnar joint is formed between the sigmoid notch found along ulnar border of distal radius and the ulnar head. The joint is mainly stabilized by volar and dorsal radioulnar ligaments which function as the primary stabilizers of the DRUJ.
The distal radioulnar joint is most stable in supination
The conventional mechanism of injury is thought to be axial loading of the forearm along with rotation. Rotation is often pronation but supination is also known to be associated. hyper pronation of the forearm. But till now, the injury could not be reproduced in the lab so the exact forces are yet to be worked out.
Direct blows on the dorsolateral side are also known mechanism of Galeazzi fracture injury.
The deforming forces in a Galeazzi fracture include
- Brachioradialis
- Pronator quadratus
- Thumb extensors
- Weight of the hand
Walsh classification of Galeazzi Fracture
This classification is based on the position of the radius after injury
Type I
- dorsal displacement of the radius
- Supination force
Type II
- Volar displacement of the radius
- Due to pronation force
Clinical Presentation
There is a complaint of swelling in the distal third of the radius and wrist joint.
Pain and soft-tissue swelling are present at the distal-third radial fracture site and at the wrist joint.
There is tenderness in the same area.
The function of the elbow joint should be assessed. The distal neurovascular examination should be done.
Anterior interosseous nerve, a division of the median nerve, can be injured with Galeazzi fracture.
This nerve affects the function of the flexor pollicis longus and flexor digitorum profundus to the index finger.
Imaging
The xrays help to determine the level of the fracture, configuration of the fracture and associated distal radioulnar joint injury.
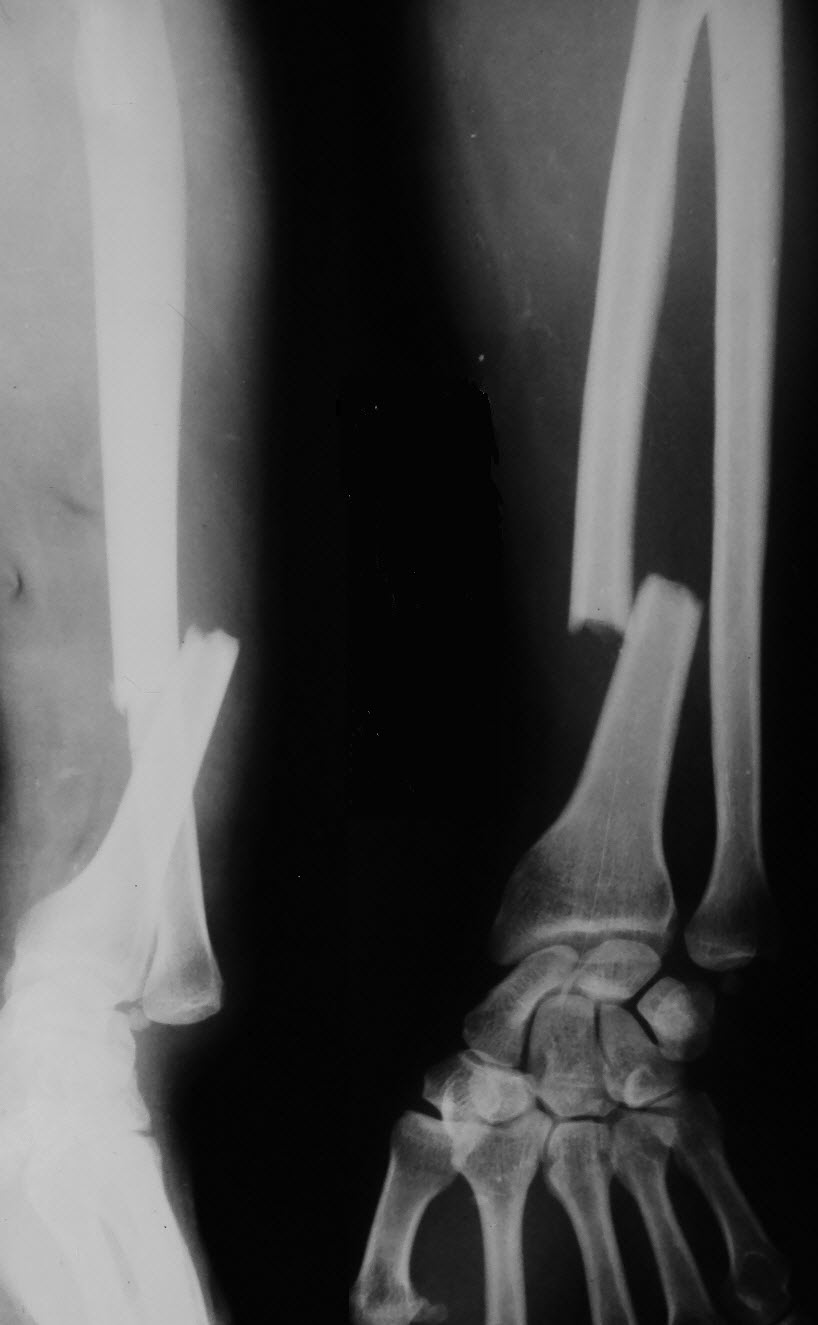
Anteroposterior and lateral view of forearm including elbow and wrist joint are sufficient to evaluate the injury.

Following findings are noted
- Radial fracture site
- Angulation
- Degree of shortening
- Distal radioulnar joint dislocation
Radial shaft fracture is commonly seen commonly at the junction of the middle and distal third. There is usually dorsal angulation.
There would be a dislocation of the distal radioulnar joint which is most notable on the lateral view. If the frank dislocation is not present, the following signs can indicate an injury to the distal radioulnar joint-
- Ulnar styloid fracture at the base
- Widening of the distal radioulnar joint on AP view
- A comparison with the opposite wrist would help
- Radius shortening by more than 5 mm relative to the distal ulna
- If greater than 10 mm, suggests complete disruption of the interosseous membrane
Sometimes, the assessment of the distal radioulnar joint is difficult with plain radiography alone.
Bilateral axial computed tomography of the forearm is the preferred study for analyzing distal radioulnar joint injury.
In addition to stating the presence of the radial fracture and distal radio-ulnar joint dislocation, a number of features should be sought and commented on:
Radiographs of the contralateral extremity can be obtained for comparison.
Treatment of Galeazzi Fracture
In adults, the treatment of choice is surgical as the fractures do not yield good results with closed reduction and plaster cast application.
Open reduction and internal fixation using plate and screws is the preferred treatment. The distal radioulnar joint should be assessed after the fixation and if required can be given a temporary stabilization by K-wire.
The implant of choice for Galeazzi fracture is limited contact dynamic compression plate and 3.5 mm screws.
Using the dorsal or volar approach, the radius fragments are exposed and reduced. The fracture is fixed with the implant of the suitable size usually 6 or 7 hole plates maybe 5 holes in case one fragment is very small.
If the joint is reducible but unstable, then the position of maximum stability should be found and limb should be splinted in that position. The splint is continued for 4 weeks after the injury and the mobilization of the limb should begin. Night splinting in a stable position should continue until 3 months after injury.
If no stable position can be found, the distal radioulnar joint should be stabilized with a radioulnar pin for 3 weeks. Alternatively, a screw can be used if greater stabilization is needed. The problem with screw is difficult removal.
Very rarely the joint may not be reducible at all. This usually happens in case of malreduction of the radius or soft tissue interposition within the joint.
If the reduction is anatomic and joint is not reducible, open reduction of the distal radioulnar joint is required.
In children, Galeazzire fractures patients are typically treated with closed reduction and casting as their bones are more plastic and there is stout.
Thus, closed reduction with long arm casting is the first line of treatment in children. Both radius and distal radioulnar joint should be anatomically reduced.
The fractures which do not reduce well are treated by open reduction and internal fixation of radius along with distal radioulnar joint pinning. Rradial fixation can be done with volar plate or flexible intramedullary nail.
Complications
- Nonunion/Malunion
- Infection
- Refracture following plate removal
- Nerve injury
- Radial sensory nerve
- Posterior interosseous nerve injury
- Ulnar nerve
- Instability of the DRUJ
Ulnar nerve injury, though rare, has been reported
Failure to recognize injury or improper reduction could lead to chronic instability.
Prognosis
Successful of the treatment depends on the reduction of the radius and distal radioulnar joint.
The incidence of nonunion of Galeazzi fractures is very low.
References
- Atesok KI, Jupiter JB, Weiss AP. Galeazzi fracture. J Am Acad Orthop Surg. 2011 Oct. 19 (10):623-33.
- Ploegmakers JJ, The B, Brutty M, Ackland TR, Wang AW. The effect of a Galeazzi fracture on the strength of pronation and supination two years after surgical treatment. Bone Joint J. 2013 Nov. 95-B (11):1508-13.
- Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin. 2007 May. 23 (2):153-63.