Last Updated on August 2, 2019
Ganglion cyst is the most common benign tumor of the hand. It is thought to be degeneration of the mucoid connective tissue.
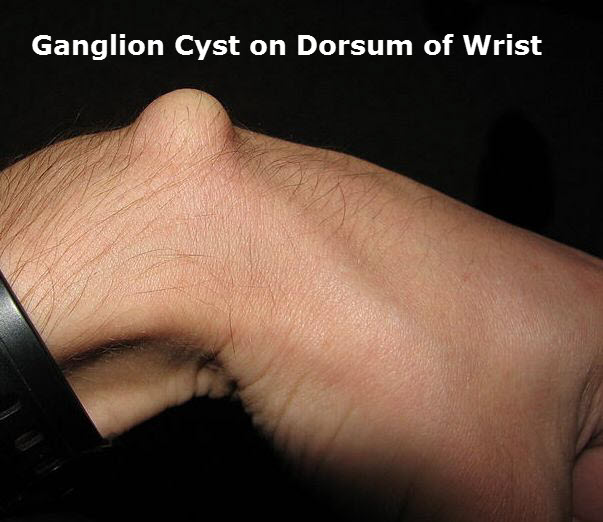
It most commonly occurs on the dorsal wrist in 60% cases and is seen as bump on the wrist.This arises generally from scapholunate joint but can also arise from the radioscaphoid or scaphotrapezial joint in which case the presentation is on volar aspect. When located at the distal interphalangeal joints, they are termed mucous cysts.
A ganglion cyst is also known as Gideon’s Disease, a Bible Cyst, or a Bible bump.
Ganglion cyst is a fluid-filled cyst which can quickly appear, disappear, and change size.
Mostly asymptomatic, ganglion cyst causes symptoms of pain, stiffness and weakness.
In cases where compression of the nerve occurs [median/ulnar nerve] paraesthesiae may be reported.
These occur three times as often in women as they do in men.
Ganglion cysts within the bone, termed interosseous cysts, most often affect the scaphoid and lunate and require open surgery for removal; therefore, it is important to determine whether the cyst is the cause of the pain.
Pathophysiology of Ganglion Cyst
A ganglion rises out of a joint, like a balloon on a stalk. It grows out of the tissues and contains fluid.
The cause of the ganglion cyst has been described as an outpouching of synovium which probably results from an irritation of articular tissue. This irritation is thought to cause
- New tissue formation
- Degeneration of connective tissue
- Cystic space formation
- Mucin production by mesenchymal cells
Most of the ganglion cysts are multiseptate.
A major component of the fluid is hyaluronic acid. Collagen fibers and fibrocytes make up the wall lining. The ganglion cyst is thought to begin as swelling of collagen fibers and fibrocytes, followed by degeneration and liquefaction of these elements. Lastly, the proliferation of connective tissue occurs.
Clinical Presentation
The cysts can occur at any joint or tendon sheath. Dorsal aspect of the wrist followed by the volar aspect of the wrist are most commonly affected. Other common sites are foot, ankle, and knee.
They can also be present in the flexor tendon sheath.
The swelling itself is the main concern of the patient who seeks medical help. Sometimes the swelling could be therefore a long time before someone seeks advice, often due to recent development of pain or limitation of activity.
On examination, the skin over the cyst is normal. The cyst mass is compressible, could be mobile to some extent and transillumination is possible.
Mucous cyst is the name given to ganglion cyst at distal interphalangeal joint. This may be associated with osteoarthritis of the hand. There may be thinning of the overlying skin and nail malformation.
Lab Tests
Lab tests do not show any abnormality and are not required for the diagnosis
Imaging Studies
Xray is useful to show bony abnormalities that may be causing the symptoms or may contraindicate treatment.
Magnetic resonance imaging, ultrasonography, or arthroscopic imaging may prove useful in obtaining confirmation of clinical diagnostic findings to confirm clinical findings.
Treatment of Ganglion Cyst
Pain, limitation of movement, and nerve involvement [Compression of the sensory or motor median nerve cutaneous branches in case of volar wrist ganglion] are indications for surgical removal of the cyst. If the cyst is being treated for cosmetics or aesthetic reason, nonoperative methods are chosen.
Non-Operative Treatment
Observation
Most of the ganglion cysts do not have symptoms. Just waiting and watching may be advised to make sure that no abnormal changes are occurring.
Immobilization.
A wrist brace or splint may relieve symptoms and cause the ganglion to decrease in size.
Repeated Aspiration with or without Steroid Instillation
Repeated aspiration with or without instillation of steroid can help ganglion cyst. Minimum of 3 aspirations help to reach a cure rate of 85%.
Corticosteroid instillation is controversial at the moment, with some preferring and others not.
Removal of Ganglion Cyst
Removal of the cyst could be done as an open procedure or arthroscopically. Recurrence, up to 40% is noted irrespective of the treatment procedure.
Removal of the stalk, when visualized or removal of the origin of cyst further decreases the chances of recurrence.
When a portion of the capsule is removed as well, recurrence rates decrease to as low as 4%.
A volar ganglion cyst is much more likely to recur than a dorsal ganglion cyst.
Arthroscopy uses smaller incisions, allows better visualization and easier identification of other intra-articular pathologies.
For volar ganglion cysts, an open procedure is usually preferred.
When operating for mucous cyst, it is important to remove osteophytes too, to reduce the rate of recurrence.
In open and arthroscopic procedures, wrist stiffness is the most common postoperative complication.
Neurovascular injury is a possible complication.
Prognosis
Recurrence is problem after removal.
Role of Bashing or Blunt Trauma in Treatment of Ganglion
Recent studies have suggested that using blunt force or bashing could be effective treatment for ganglion.