Last Updated on November 19, 2023
Hip biomechanics are complex because of the pelvic motion associated with it and the wide range of movements it undergoes in daily routine. Biomechanics is the science that studies forces acting on a living body.
The hip is a ball-and-socket joint that balances the body weight during stance and gait. It is quite peculiar of this joint that it is never fully unloaded.
The stability of the joint is contributed by articular shapes and the integrity of the soft tissues.
The stability of this joint is critical to allow motion while supporting the forces encountered during daily activity. Nearly all motion between the femoral head and acetabulum is rotational, with no detectable translation because of the congruency of the articulating surfaces.
Understanding hip biomechanics is important for understanding the effect of many diseases on the activities involving the hip and planning treatment. Hip biomechanics also have a major role to play in designing the prosthesis for hip replacement.
Relevant Anatomy
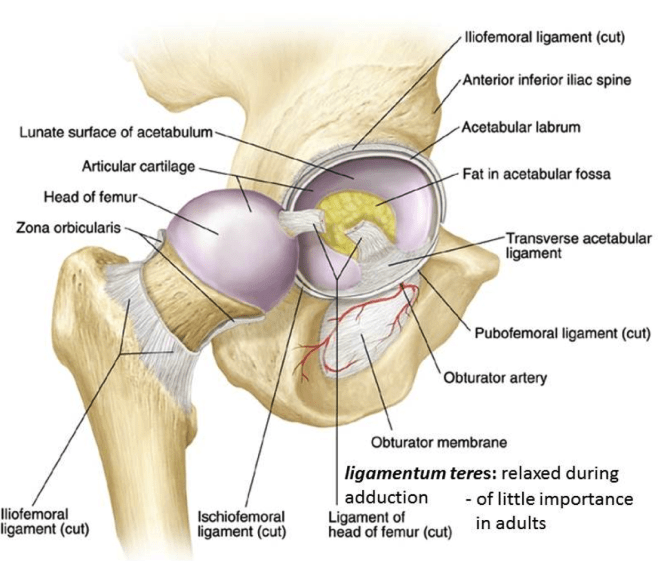
Hip is a mobile and stable joint because of its anatomy and strong attachments of muscles and ligaments. It is a ball-and-socket joint with movements in sagittal, frontal, and transverse planes.
The shape of the head of the femur is described not as an exact sphere but conchoid or ellipsoid. This shape is thought to make the hip joint more stable and less likely to subluxate. The horseshoe geometry of the acetabular cartilage has been shown to optimize the stress distribution.
The neck of the femur and its orientation plays an important role in the mobility of the hip. The neck is angulated in relation to the femur in the sagittal and coronal plane.
Neck-shaft angle is about 140 degrees at birth and reduces to 120-135 degrees in adults.
The anteversion is about 40 degrees at birth but reduces to 13-16 degrees in adults.
The orientation of the acetabulum is also important for hip stability and transfer of the forces. It is directed forward 15-20 degrees and 45 degrees downwards.
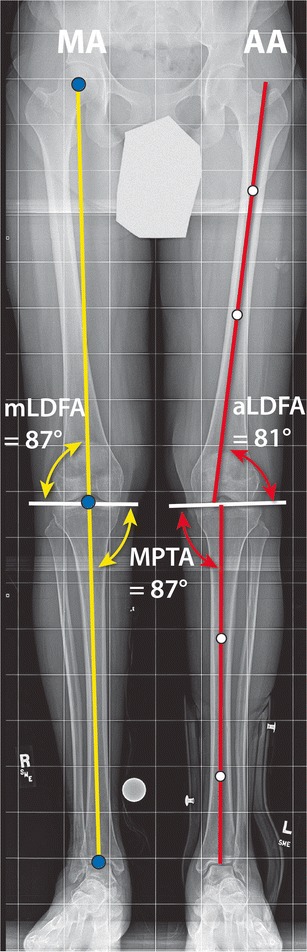
The mechanical axis of the lower limb passes between the center of the hip joint and the center of the ankle joint.
The anatomical axis line is between the tip of the greater trochanter to the center of the knee joint.
There is about 7 degrees of angle between the two axes.
Movements of Hip
[Read about Muscles of the Hip]
The hip is most mobile in the flexion. it can reach about 100 degrees of flexion with an extended knee and 140 degrees when the knee is flexed too.
The movement of extension is only 15-20 degrees.
Hips can have about 45 degrees of abduction and 30 degrees of adduction. External and internal rotations are 15-20 degrees respectively.
Variations in the range may exist across individuals and ages.
During the walking or gait cycle, the hip goes through following in various phases of the gait
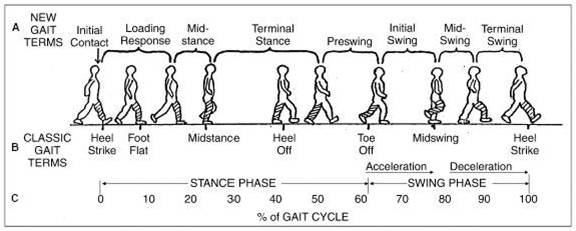
- Maximally flexed (35–45 degrees ) during the late swing phase of gait, as the limb moves forward for a heel strike.
- Extends as the body moves forward with maximum extension at heel-off.
These movements are noticeable in the sagittal plane but other movements accompany these as follows-
- Abduction– During the swing phase of gait and reaches a maximum just after toe-off.
- Adduction– Occurs at the heel strike and is maintained during the stance phase.
- Externally rotated during the swing phase
- Internal rotation at foot strike
- Gradually goes away as the opposite hip moves forward
The movements of the hip are well coordinated with the pelvis and therefore it is important to understand their dynamic relations.
Hip, Pelvis and Spine Interplay
For an upright posture, the lateral view of the center of the hip must lie under the center of the spine. This is maintained by the interplay of sacral slop and pelvic tilt. This dynamic relationship between these structures moves in a predictable way to maintain sagittal balance.
[Read more about pelvic tilt and sacral slope]
For example, if there is an increase in lordosis i.e. sacral slope increases, the pelvis would accommodate by decreasing the pelvis tilt [or by pelvic flexion]cetabular orientation is not fixed.
The sum of pelvic tilt and sacral slope is called pelvic incidence. While both pelvic tilt and sacral slope change with body position pelvic incidence remains the same.
For example, when standing – -lumbar lordosis and thus sacral slope increases, and the pelvis tilts forward [flexes] decrease in a pelvic tilt.
During sitting, the pelvis tilts backward (ie extends) causing increased pelvic tilt that causes increased acetabular anteversion as acetabular orientation changes with a change in pelvic position. During sitting, the lumbar lordosis decreases thereby causing a decrease in sacral slope.

Movements of Pelvis with Hip Movements
- Flexion
- Iliopsoas muscle, rectus femoris, and others
- This can result in anterior tilting of the pelvis if the abdominals are weak
- This may result in exaggerated lumbar lordosis
- Extension
- Gluteus Maximus, posterior head of adductor magnus, and hamstring muscles
- Results in posterior tilt
- Reduction of natural lordosis
- Abduction
- Gluteus medius, gluteus minimus, tensor fasciae latae and others
- When the pelvis is stabilized, abductor muscles lead to hip abduction
- During gait, abductors have an important role in the stabilization of the pelvis in a single-limb stance
- Need to produce almost double the force than body weight to keep the pelvis stable [detailed discussion later]
- Adduction
- Pectineus, adductor group, gracilis and others
- When the pelvis is stabilized adductors lead to adduction of the limb
- During rapid or complex movements adductors participate in femoral on pelvis and pelvis on femur stabilization
- External Rotation
- Gluteus Maximus and short external rotators
- Lead to external rotation of the femur over the acetabulum when the pelvis is stable
- Can contribute to pelvic rotation when the femur is fixed
- This helps in changing direction while running
- Internal Rotation
- Anterior fibers of gluteus medius and minimus, parts of 3 adductor muscles, TFL
- Act in opposition to external rotators
Forces Acting on the Hip
Force is generated within a joint in response to forces acting on the joint in the hip. It is called the joint reaction force and balances the arms of the body weight and abductor tension that maintains the pelvis at level.
Joint reactive forces depend on the activity. The joint reaction force is measured in terms of body weight. For example, walking produces 2.5 times reaction force whereas running produces 6-8 times.
The center of gravity is the average location of the weight of an object. In humans, it is just anterior to S2.
The hip joint is the first-class lever. In a first-class lever, the fulcrum is placed between the effort and load.
The fulcrum here is hip and the load is body weight. Abductor tension is the effort.
To maintain a stable hip, the torques that are produced by the body weight are opposed by the pull of the abductor muscles. [see the diagram below]
Abductor force x lever arm A = weight x lever arm

Thus the forces acting across the hip joint are
- Body weight
- Abductor muscle force
- Joint reaction force
The body lever arm and the abductor muscles lever arm have a ratio of 2.5:1. That means that in a single-leg stance, hip abductors need to generate two times the body weight’s force to maintain balance and prevent dropping of the pelvis on the opposite side.
Recent studies have supported the role of the iliotibial band in hip stability. It serves as a tension band to relieve the gluteus medius during the midstance phase of gait
Two Leg Stance
During a two-leg stance, the center of gravity is located between the two hips, with an equal force exerted on both hips. Each hip roughly supports the weight of the upper body equally on the femoral heads. Each hip supports about one-third of body weight.

Thus, the weight of the upper body is equally divided on both hips and there is little need for muscular force.
Single Leg Stance
During the single-leg stance, this force is 3 times body weight. The limb on which weight is supported would have to bear the upper body weight and the contralateral, non-supporting limb.
The effective center of gravity shifts to the non-supportive leg and distally.
This leads to a downward force that attempts to tilt the pelvis on the unsupported side.
The abductors on the hip of weight bearing limb must exert a downward counterbalancing force with the right hip joint acting as a fulcrum. The ratio of the length of the lever arm of the body weight to that of the abductor musculature is about 2.5: 1. Therefore the force needed by abductor muscles must approximate 2.5 times the body weight to become equal to the force applied by body weight.
This force by abductors must be equal to the load applied by weight to hold the pelvis level when in a one-legged stance and a greater moment to tilt the pelvis to the same side when walking.
Weakness of abductors may lead to dropping of the pelvis on non wt-bearing side.
The estimated load on the femoral head in the stance phase of gait is equal to the sum of the forces created by the abductors and the body weight and is at least three times the body weight.
- Roughly, the joint reaction force would be equal to the sum of body weight and abductor force.
- During walking it is 5 times and during running it is 10 times.
- Getting on & off the pan puts a load equal to four times body weight.
The use of the cane may relieve up to 60% of the load on the hip in the stance phase because the can transmits the weight to the ground and results in lesser force required to counterbalance.
Hip Biomechanics During Gait
During normal gait, on heel-strike, the hip moves into 30 degrees of flexion and at toe-off [when the foot is finally off the ground] about 10° of extension. The range of abduction to adduction is about 11°, and for internal-external rotation, the range is about 8°.
During different phases of the gait cycle, different forces act on the femoral head. Approximately two-thirds of the hip force is produced by the abductors.
It is useful to consider the forces relative to axes based on the long axis of the femur.
In the coronal plane, the forces acting make an angle of 15° to 27° to the long axis of the femur during the stance phase of gait which results in axial compression, varus, and mediolateral forces. In the sagittal plane, anteroposterior forces on the femoral head, result in torsion.
Factors Affecting Hip Biomechanics
Shortening of the abductor lever arm
Shortening of the abductor lever arm would result in an increase in abductor workout. The abductor lever arm may be shortened in
- Arthritis
- Supratrochanteric shortening
- Femoral anteversion
- External rotational deformities
- Developmental dysplasia of the hip.
If the muscles are not able to generate the requisite force to counterbalance body weight, it would result in a lurch during the gait or pelvic tilt.
Weight Gain
We have seen that forces acting on the hip are measured as multiples of body weight. Therefore, the increase in weight leads to an increase in forces acting on the joint.
Use of Hip Biomechanics in Clinical Scenario
Hip Pain
- painful hip management requires a reduction of the joint reaction force. This can be achieved by the following:
• Weight loss - Strengthening the abductor’s muscles
- Bringing the center of gravity closer to the center and thus reducing the moment arm. This can be achieved by using a cane in the opposite hand. When 15 percent of weight is through the cane, there is a decrease in joint reaction force by 50 percent. This occurs because the cane has a longer moment arm. This results in lesser strain on abductor muscles.
Prosthesis Design
Hip biomechanics are used in the designing of hip prostheses. The idea of the design is to decrease the joint force by
- Centralization of femoral head by deepening of Acetabulum – decreases body wt lever arm
- Increase in neck length and lateral reattachment of trochanter – lengthens abductor lever arm
Articular clearance and cup orientation are other important parameters in prosthetic hip biomechanics.
This aims at decreasing abductor force, and joint reaction force, & so the wear of the implants.
Femoral offset is the distance between the center of the head to the center of the axis of the stem
An inadequate medial offset shortens the moment arm leading to increased abductor work. It could lead to limp and increased bony impingement.
Errors in femoral stem implantation alter the hip biomechanics. Varus or valgus positioning may either increase or decrease the femoral offset and abductor lever arm.
Femoral offset is the distance from the center of rotation of the femoral head to a line bisecting the long axis of the femur.

If the offset is increased, there is increased stress on the stem which leads to implant loosening. This is because as an increase in offset would increase in the bending moment on the stem.
A decrease in femoral offset would move the femur closer to the pelvis medially. This can lead to the impingement of greater trochanter in extremes
In the sagittal plane, the forces act to bend the stem posteriorly and become more pronounced when the hip is flexed. It has been found that the joint reaction force was lower when the hip center was placed in the anatomical location compared with a superior and lateral or posterior position.
References
- Menschik F. The hip joint as a conchoid shape. J Biomech. 1997;30(9):971–3. [Link]
- Fetto J, Leali A, Moroz A. Evolution of the Koch model of the biomechanics of the hip: a clinical perspective. J Orthop Sci. 2002;7(6):724-30.
- Fetto JF. A dynamic model of hip joint biomechanics: The contribution of soft tissues. Advances in Orthopedics. 2019 Jun 4;2019.
- D’Lima, D.D., et al., The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am, 2000. 82(3): p. 315-21.