Last Updated on October 28, 2023
A hip pointer refers to a contusion to the iliac crest or the greater trochanter of the femur caused typically by a direct blow or fall. Other involved structures may include the tensor fascia lata, the external oblique muscle and the greater trochanter of the femur.
Severe cases may have In severe cases a hematoma, causing palpable fluctuant mass beneath the skin.
{kind=link}
Hip pointers are often seen in contact sports like volleyball, football or ice hockey. A fall on the hip could also be responsible.
Incidence statistics for hip pointers are not available.
Functional Anatomy
Read anatomy of upper end of femur
The iliac crest is the superficial bony prominence felt beneath the skin on either side at the level where a wearable belt is.
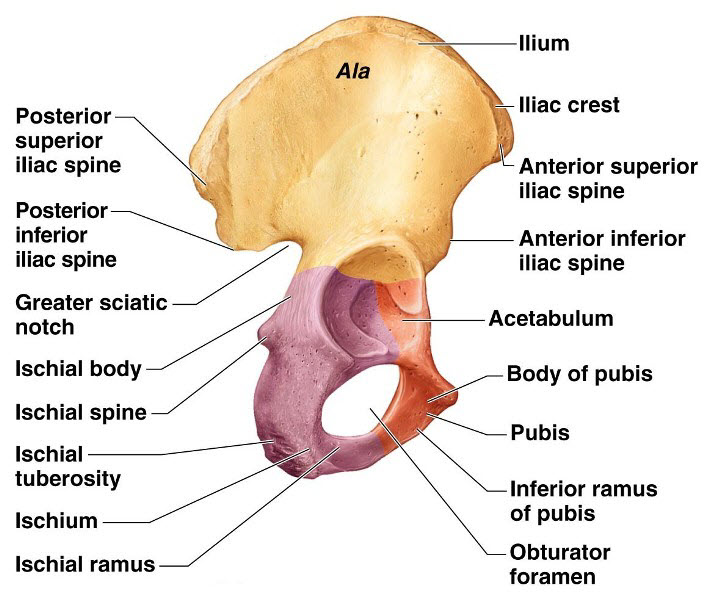
It is a part of the pelvic girdle.

It serves as attachments for many muscles, including the internal and external obliques, the tensor fascia lata, the gluteus medius, the latissimus dorsi, and the paraspinal muscles.
Because of the minimum tissue covering, the anterior iliac crest region of the hip and the greater trochanter of the femur are more susceptible to contusion and injury than more protected regions of the body.
Cause of Hip Pointer
Hip pointers are caused by a sudden impact that’s hard enough to bruise your iliac crest or greater trochanter or cause damage to the soft tissue of your hip.
Some of the more common causes of hip pointers include:
- Sports that involve direct physical contact. An incomplete list is
- Football,
- Rugby
- Martial arts
- Hockey
- Baseball
- Football
- Sports that are played on hard surfaces [a hard landing on asphalt or a gym floor can cause a hip pointer.]
-
- Volleyball
- Basketball
- Skateboarding
- Sports that can involve crashes.
- Skiing
- Snowboarding
- Cycling
- Inline skating.
What Are the Symptoms of a Hip Pointer – Clinical Presentation
The severity of the injury determines the severity of the symptoms.
Most hip pointers cause mild symptoms and often the patient does not seek medical advice.
The patient presents with the sudden onset of hip pain in the iliac crest or greater trochanteric. There would be a history of trauma suggesting an injury to the region.
The pain is well localized and often exacerbated with activities such as running, jumping, twisting, or bending.
Depending on the associated muscles involved, the patient may find it difficult to move the hip or rotate the trunk.
Bruising and hematoma may be noticed and examination may reveal muscle spasm.
Presence of hematoma is associated with severe pain, as it dissects between the gluteus muscle and the iliac crest and can potentially press on the femoral or lateral femoral cutaneous nerves.
Abdominal examination to exclude trauma to intra-abdominal organs should be done.
The motor strength of the hip flexor and extensors is normal, though the hip abductors and external rotators function may be limited by pain if the contusion includes the sartorius muscle and/or the iliotibial tract.
The neurovascular examination is normal.
Differential Diagnoses
- Chronic Exertional Compartment Syndrome
- Hip Injuries
- Hip Tendonitis and Bursitis
- Iliotibial Band Syndrome
- Osteitis Pubis
- Sacroiliac Joint Injury
- Slipped Capital Femoral Epiphysis
- Snapping Hip Syndrome
Laboratory Studies
Laboratory studies are not useful in the diagnosis of hip pointers.
Imaging Studies
X-rays are done in case a fracture is suspected.
CT scan is done if the patient has continued pain or if the pain is disproportionate to examination findings.
CT scans can help to diagnose deep hematoma or internal visceral injuries.
A bone scan can be ordered to rule any stress fracture in cases where the initial radiographic findings are normal and the symptoms do not resolve or improve.
Treatment of Hip Pointer
Acute Phase
Initial therapy of a hip pointer injury consists of
- RICE therapy
- NSAIDs
- Restriction of activity
- Rest to part
Crutches can be used to assist in walking.
If a significant hematoma is present, then aspiration can be done. Aspiration relieves the pain and also prevents the development of myositis ossificans or compression of local nerves.
Corticosteroid injections may provide relief if greater trochanteric bursitis develops.
After a few days, when the pain decreases, the range of motion and active resistance exercises for the hip may be started. Patients may also begin the strength exercises and aerobic conditioning, as tolerated.
Patients with hip pointer injuries may return to play once pain and swelling allow a return to normal or near-normal function. Padding over the affected area may help protect the area from reinjury.
Complications of Hip Pointer
Hematoma formation may lead to myositis ossificans and scar-tissue formation.
Chronic trochanteric bursitis may develop.
Prevention of Hip Pointer
It can be difficult to prevent a hip pointer. They happen suddenly and can be difficult to see coming but extra padding and protection over the iliac crest may decrease the frequency and severity of the injury.
Prognosis
The prognosis is very good.
The player can return to the game 1-3 weeks, depending upon the extent of the injury.
References
- Hall M, Anderson J. Hip pointers. Clin Sports Med. 2013 Apr. 32(2):325-30.
- Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005-2007. Am J Sports Med. 2008 Dec. 36(12):2328-35.
- Adkins SB 3rd, Figler RA. Hip pain in athletes. Am Fam Physician. 2000 Apr 1. 61(7):2109-18.
- Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001 Jul-Aug. 29(4):521-33