Last Updated on August 1, 2019
Iliopsoas tendonitis or tendinitis is an inflammation of the tendon or surrounding tissue caused mainly by acute trauma and overuse due to repetitive hip flexion. Iliopsoas tendinitis and iliopsoas bursitis are closely interrelated because inflammation of one inevitably causes inflammation of the other because of the proximity of two structures.
These two conditions are also identical in presentation and management.
Iliopsoas tendonitis is a relatively uncommon and cause of anterior hip or groin pain and affects young adults more commonly. Females are slightly more affected.
Relevant Anatomy
[Read Anatomy of Pelvis]
[Read Anatomy of hip ]
The psoas and iliacus muscles originate from the lumbar spine and pelvis and converge to form the iliopsoas muscle, which inserts onto the lesser trochanter. The iliopsoas muscle passes anterior to the pelvic brim and hip capsule in a groove between the anterior inferior iliac spine laterally and iliopectineal eminence medially.
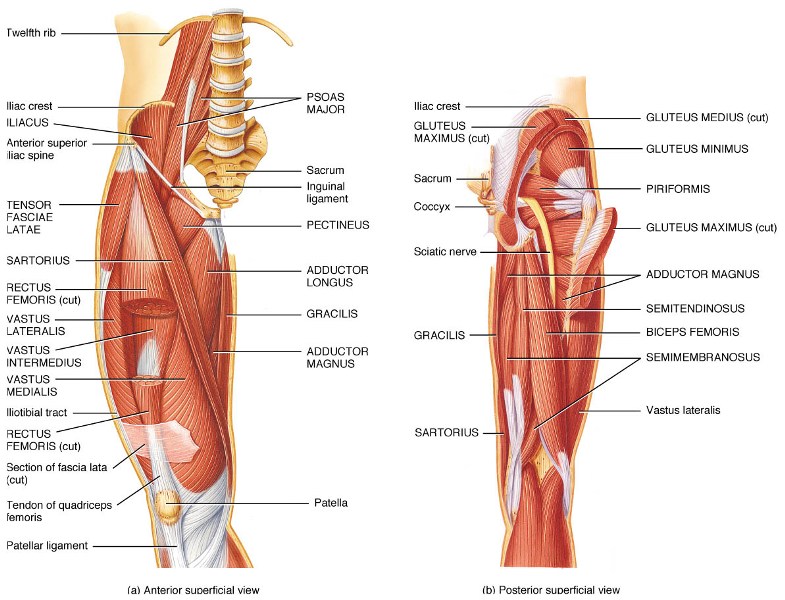
The iliopsoas muscle acts as the hip flexor and external rotator of the femur.
Pathophysiology of Iliopsoas Tendonitis
The acute injury of iliopsoas muscle usually occurs due to a sudden contraction of the iliopsoas muscle or direct trauma.
Repeated hip flexion or external rotation of the thigh is the usual cause of overuse injury and occurs in activities like dancing, running, resistance training, football, and gymnastics.
One of the factors in adolescence is that hip flexors become relatively stiff leading to increased stress on iliopsoas. This can lead to inhibition of the gluteus maximus, allowing for an anterior pelvic tilt. This leads to exaggerated lordosis and puts stress on the spine. Increased knee flexion occurs at the heel strike and during midstance phases of the gait cycle predisposing to patellofemoral problems.
Causes of Iliopsoas Tendonitis
- Rheumatoid arthritis is a cause of iliopsoas bursitis which may lead to iliopsoas tendonitis
- Injury
- Overuse
- Snapping Hip Syndrome
Presentation of Iliopsoas Tendonitis
Patients often present with complaints of an insidious onset of groin pain on the anterior aspect. Initially, the pain is present after the aggravating activity and relieved with rest. As the condition progresses, the pain is present during activity and relieved with rest.
Eventually, the pain is present during the activity and at rest as well.
The activities which aggravate pain are
- Jogging
- Brisk walking
- Running
- Kicking
- Putting on socks and shoes
- Rising from a seated position after a period
- Walking up stairs or inclines
The pain may radiate down the anterior thigh toward the knee. Audible snap or click in the hip are reported [Snapping hip syndrome]
The patient may also complain of anterior knee pain due to alteration of patellofemoral dynamics.
On examination, the affected hip may be held in slight flexion and external rotation to ease tension in iliopsoas. The patient may walk with a shorter stride on the affected side.
Anterior pelvic tilt may be there. There would be tenderness in around the insertion of iliopsoas tendon.
Ludloff Sign
The patient is asked to sit with the knee in extension and asked to lift the heel on the affected side. Pain caused by this maneuver (a positive Lu is consistent with an iliopsoas tendonitis because the iliopsoas is the sole hip flexor activated in this position.
Snapping hip sign or Extension test
The affected hip is placed in flexed, abducted, and externally rotated position. The knee is also kept in flexion to make the test easy. Now the hip is passively moved into extension. This may result in an audible snap or palpable click over the inguinal region. Associated pain is highly suggestive of iliopsoas tendonitis or bursitis.
Lab Studies
Laboratory studies are rarely required.
In such cases following investigations may be conducted
- CBC count
- ESR
- CRP
- Rheumatoid factor
- Anticyclic citrullinated peptide antibody
- Antinuclear antibody
- Urine examination.
Imaging
Xrays typically are normal but may demonstrate other bony pathologies contributing to the condition.
Ultrasound shows thickened tendon and it may show findings suggestive of iliopsoas bursitis, which may coexist.
MRI is able to differentiate between bursitis, peritendintis, tendonitis and assesses the injury better.
Lidocaine Challenge Test
This test can be done to confirm the diagnosis of iliopsoas tendonitis especially in cases where the cause of pain could not be determined with certainty. It involves an injection of 1% lidocaine under ultrasound guidance. If symptoms are relieved, the diagnosis is confirmed.
Treatment of Iliopsoas Tendonitis
Ice
Ice application is done for about 20 minutes about 3-4 times a day. It helps to relieve the pain, swelling, and inflammation.
Rest
The patient is put on a relative rest. All the activities that worsen pain are stopped. The patient is put on assisted walking with crutches
Stretch Exercise
Gentle stretch exercises reduce spasm in the iliopsoas. These should be initially done under supervision.+
Drugs
NSAIDs are used to reduce inflammation, swelling, and pain. A peritendinous corticosteroid and lidocaine may be injected under ultrasonographic guidance.
Rehabilitation Phase begins when the patient is relatively pain-free. The purpose is to regain normal range of motion, strength, and endurance. The measures include
- Iliopsoas range of motion stretch
- Rectus femoris stretch.
- Hamstring stretch [Provides a posterior counter force to iliopsoas pull]
- Strengthening of external rotators and abdominals
- Low resistance endurance
After the patient tolerates the activity, the patient should move to easy resistance cycling, walking, and jogging. After that patient may return to sport-specific activities.
Return to play is allowed when the patient is free of pain and has demonstrated adequate flexibility and strength.
Surgical Intervention
Surgical intervention is not commonly used for iliopsoas tendinitis. A partial or complete release of iliopsoas tendon, either open or arthroscopically can be considered in treatment failures.
Complications of Iliopsoas Tendonitis
Recurrence of tendonitis is a potential complication.