Last Updated on September 9, 2022
Leri Weill Dyschondrosteosis is a type of genetic disorder resulting in short stature. It typically causes the shortening of forearms and legs and Madelung deformity. Madelung deformity implies misalignment of radius and ulna in the wrist and is caused by a growth disturbance that retards the development of the ulnar and volar portions of the distal radial physis. There could be additional symptoms and the severity of the disease may vary from person to person.
It is also known by the names of Leri-Weill disease and Leri-Weill syndrome.
Leri Weill Dyschondrosteosis is a form of mesomelic dwarfism and was first described by Leri and Weill in 1929. Leri Weill dyschondrosteosis is characterized by
Causes of Leri Weill Dyschondrosteosis
Leri Weill dyschondrosteosis is caused by a mutation in the SHOX gene or its regulatory elements ) located on the pseudoautosomal region 1 (PAR1) of the sex chromosomes (X and Y chromosomes).
SHOX is located on the pseudoautosomal region of the X chromosome at Xp22 and the pseudoautosomal region of the Y chromosome at Yp11.
Thus SHOX is present in two identical copies.
Pseudoautosomal regions (PAR1 and PAR2) are short regions of X and Y chromosomes. These regions behave like an autosome and the genes in this region are inherited in an autosomal manner than sex-linked.
Leri-Weill dyschondrosteosis was first described in 1929 by doctors Léri and Weill.
A heterozygous mutation in the SHOX gene can result in Leri Weill dyschondrosteosis resulting in typical features.
Heterozygous implies that an individual carries a single defective gene, not both).
SHOX gene mutations are also responsible for a spectrum of related skeleta dysplasia like Langer mesomelic dysplasia.
Clinical Presentation
The signs and symptoms associated with Leri Weill dyschondrosteosis can vary from person to person.
Females are more affected than males.
ClassicallyGenerally, females appear to be affected more severely than males. The classic findings of the disorder are mesomelic shortening of the limbs, short stature, and Madelung deformity.
Leri Weill dyschondrosteosis is characterized by
- Variable short stature
- Short upper and lower limbs [mesomelic shortenig]
- Madelung deformity
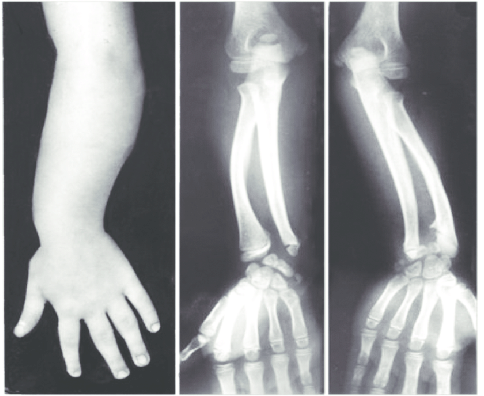
Image credit: ResearchGate
Not all individuals have Madelung deformity and many patients may attain normal heights.
Short Stature
The height of these patients is usually is less than the 25th percentile. The features become more pronounced clinically during adolescence. The degree of short stature varies from one person to other.
Mesomelic Shortening
There is a disproportionate shortening of forearms and lower legs as compared to the upper arms and legs. As a consequence, there is a disproportional shortening of limbs in relation to the trunk.
There could be abnormal bowing of the radius, ulna, and tibia as well. Consequently, the arms and legs are disproportionate to the trunk of the body. Sometimes, the shin bone (tibia) and the lower arm (radius and ulna) may be abnormally bowed. Less often, wrist, knee, and/or ankle pain may occur.
The shortening of limbs is noted first in school-aged children and can increase in frequency and severity with age.
Madelung Deformity
The primary deformity is bowing of the distal end of the radius, which is the most typical form curves in a volar direction while the ulna grows in a straight line. The distal ends of the radius and ulna are at different levels in the lateral plane. That of the ulna has maintained its original normal position, while that of the radius has curved down to a volar level.
One of the differentiating features is that the proximal radius is involved in patients with Leri Weill dyschondrosteosis whereas it is not involved in primary Madelung deformity.
Generally, bilateral Madelung deformity is seen.
Not all patients of Leri Weill dyschondrosteosis have Madelung defromity.

In addition, the patient may complain of pain in various joints.
Other features that may be present are
- High arched palate
- short, thick metacarpals
- Scoliosis
- Calf hypertrophy
Diagnosis of Leri Weill Dyschondrsteosis
The diagnosis is based on
- Clinical findings
- X-rays
- Molecular testing
Certain symptoms may not be apparent until puberty, making the diagnosis difficult.
X-rays can reveal characteristic changes like bowing of the bones and Madelung deformity.
Molecular genetic testing can confirm a diagnosis in as much as 70% of cases and is able to detect changes in the SHOX gene or /and its regulatory elements.
Treatment of Leri Weill Dyschondrosteosis
The treatment is symptomatic and supportive only. This includes wrist splints and treatment for joint pains.
Growth hormone therapy may be considered in children who are yet to reach puberty and is shown to improve adult height by as much as 10 cm.