Last Updated on October 28, 2023
Lower extremity functional scale is a test that consists of a questionnaire to evaluate the function of the lower limb in case of musculoskeletal condition or disorder. The test can be used to measure initial function, ongoing progress, and outcome.
The lower extremity functional scale was developed in 1999 by Binkley et al. when they were evaluating a group of patients with musculoskeletal disorders.
The areas of assessment include
- Activities of daily living
- Balance – non-vestibular coordnination
- Functional mobility
- Life participation
- Occupational performance
- Quality of life
- Range of motion and strength.
The scale is used for measuring lower extremity function in a wide variety of disorders and treatments. It can also be used in cases of the stroke where lower limb functions are affected.
It can be used to monitor the patient over time and to evaluate the effectiveness of an intervention.
The range of possible scores is 0-80, with 4 being the maximum score for each question.
Method of Evaluating the Patient – the Questionnaire
The patient is given a paper containing questions with an option to mark one of the following choices for each question.
The questionnaire contains 20 questions about a person’s ability to perform everyday tasks which include
- Any of your usual work, housework or school activities.
- Your usual hobbies, recreational or sporting activities.
- Getting into or out of the bath.
- Walking between rooms.
- Putting on your shoes or socks
- Squatting
- Lifting an object, like a bag of groceries from the floor.
- Performing heavy activities around your home
- Performing light activities around your home
- Getting into or out of a car
- Walking 2 blocks
- Walking a mile
- Going up or down 10 stairs (about 1 flight of stairs)
- Standing for 1 hour
- Sitting for 1 hour
- Running on even ground
- Running on uneven ground
- Making sharp turns while running fast
- Hopping
- Rolling over in bed
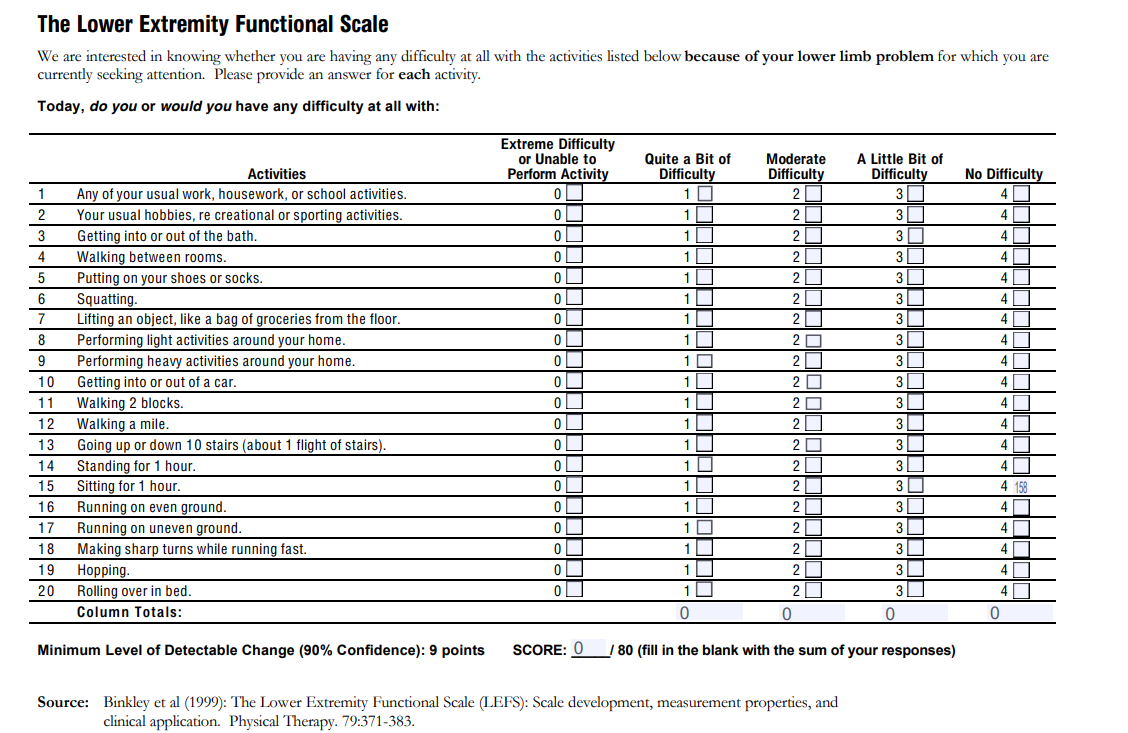
A sample questionnaire is provided in the image.
For each question, there are five possible answers with scores given accordingly
- Extreme Difficulty or Unable to Perform Activity- Score Zero
- Quite a Bit of Difficulty – Score 1
- Moderate Difficulty- Score 2
- A Little Bit of Difficulty- Score 3
- No Difficulty- Score 4
Scoring and Interpretation
A total is calculated by adding the score for individual questions.
The maximum score is 80.
The score from the individual questionnaire is calculated as a percentage
A fully functional lower limb will have score 80 and thus in % the score would be
Lower Extremity Function Score: [80 / 80]X100 = 100.0 %
In another example, a patient having score 64 would have a score as follows
[64 / 80]X100 = 80%
Thus, the higher the score, the better is the patient activity.
The lower the score the greater the disability
When doing sequentially, a minimal detectable change of 9 scale points is considered significant
The Test-retest reliability of the score has been found to be was 0.94.
The limitation of the scale is that it is not possible to assess the status of pre-disease physical function. Because the answers to the questions that pertain to past status are based on the recall and it brings in recall bias.
References
- Binkley J M, Stratford P W, Lott S A, Riddle D L. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther 1999; 79(4): 371–83.
- Stratford P, Hart D, Binkley J, Kennedy D, Alcock G, Hanna S. Interpreting lower extremity functional status scores. Physiother Can 2005; (57): 154–62.