Last Updated on August 29, 2021
Muscles of pectoral region or pectoral muscles are the muscles that connect the front of the chest to the bones of shoulder and arm.
The pectoral region refers to the anterior chest wall.
They are commonly called as pecs. These muscles also provide shape to the chest and pectoral exercises are quite famous among bodybuilders.
The following four muscles constitute the muscles of pectoral region.
- Pectoralis major
- Pectoralis minor
- Serratus anterior
- Subclavius
Between the ribs are various groups of intercostal muscles of thorax.
Let us discuss, the anatomy of pectoral muscles in detail including their origin, insertion, nerve supply and action.

Muscles of Pectoral Region
Pectoralis Major
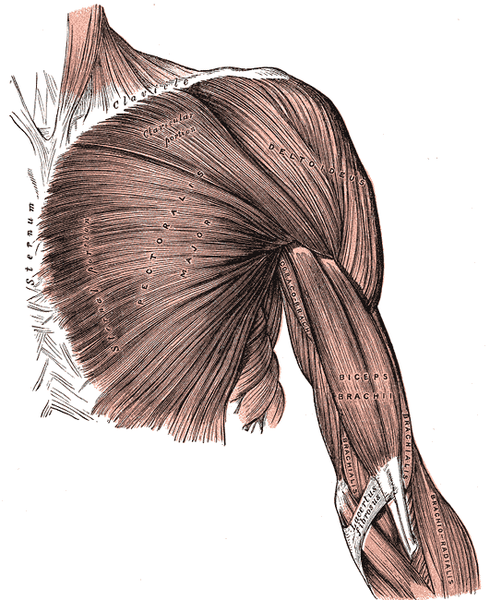
The pectoralis major is the most superficial, large, fan-shaped muscle in the pectoral region.
Origin
It is composed of two parts
- Clavicular head- originates from the anterior surface of the medial or sternal half of the clavicle.
- Sternocostal head – originates from the anterior surface of the sternum, the superior six costal cartilages and the aponeurosis of the external oblique muscle.
The fibers converge toward their insertion. Fibers arising from the clavicle pass obliquely downward and laterally. The fibers arising from the lower part of the sternum and cartilages run upward and laterally. The fibers in the middle run outward laterally. The upper fibers are usually separated from the rest by a slight interval.
Insertion
The fibers form a flat tendon which is about 2 inches and inserts into the lateral lip of the bicipital groove or intertubercular sulcus of the humerus
Pectoralis major tendon has two laminae which are usually blended together. The anterior lamina receives the clavicular and uppermost sternal fibers. The rest of the sternal fibers and coastal fibers form posterior laminae.
The posterior lamina reaches higher on the humerus than the anterior one and this gives the tendon a twisted appearance.
The distal attachment of both heads is into the intertubercular sulcus of the humerus.
Nerve Supply
Lateral [C5, 6] and medial [C7,8,T1] pectoral nerves.
- The sternal head – medial pectoral nerve.
- The clavicular – lateral pectoral nerve.
The lateral pectoral nerve is also called the lateral anterior thoracic nerve and is branch of the brachial plexus.
Read More| Anatomy of the brachial plexus
Functions
Pectoralis major adducts and medially rotates the upper limb. It also draws the scapula anteroinferior.
Acting solely, the clavicular head causes flexion of the shoulder.
Pectoralis Minor
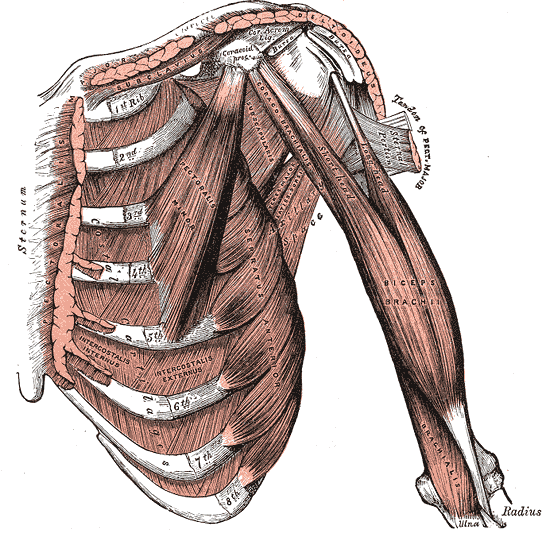
The pectoralis minor is under the pectoralis major and as the name suggests, smaller. Together, these muscles form anterior wall of the axilla region.
Origin
Pectoralis minor takes origin from 3rd-5th ribs near the costochondral junction and from the aponeuroses covering the intercostal muscles.
Insertion
The fibers go in the superior and lateral direction to converge in a flat tendon, which is inserted into the medial border and upper surface of the coracoid process of the scapula.
It inserts into the medial border and superior surface of the coracoid process of the scapula.
Nerve supply
Medial pectoral nerve [C8]
Function
Pectoralis minor muscle stabilizes the scapula by drawing it anteroinferior [down and forrward] against the thoracic wall.
It also raises the raises ribs in inspiration
Anatomically, the pectoralis minor is used as a landmark for the division of axillary artery into the first, second and third parts.
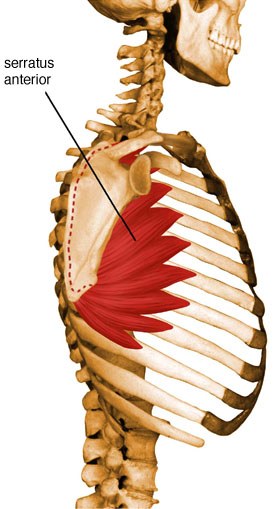
Serratus Anterior
The serratus anterior muscle is more lateral to the pectoralis minor and major. It also forms the medial border of the axilla.
Origin
The muscle takes origin by several strips [9-10] from first eight or nine ribs. Second rib contributes two slips, hence the number of slips is more than the ribs contributing.
Insertion
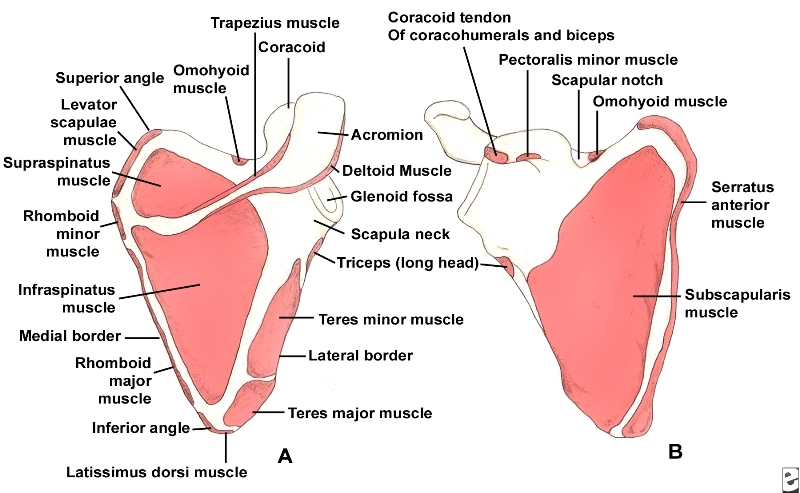
The muscle is inserted into the costal surface (the one that faces the ribs) of the medial border of the scapula. Som authors divide into three parts
- Serratus anterior superior – inserts near the superior angle
- Serratus anterior intermediate – inserts along the medial border
- Serratus anterior inferior- inserts near the inferior angle.
Nerve Supply
It is supplied by the long thoracic nerve, also called nerve of Bell. It is a branch of brachial plexus. It is prone to injury during the surgeries of the region owing to its long course over the muscle.
Function
It is a rotator of the scapula and contributes to raising of the arm beyond 90 degrees by rotating scapula. It also holds the scapula against the ribcage.
Serratus anterior, all three parts, pull the scapula forward around the thorax and this action is antagonistic of rhomboids. [Rhomboids are rhombus-shaped muscles in the back and participate in movements of scapula.]
But the inferior and superior parts acting together also keep the scapula pressed against the thorax along with the rhomboids, acting in a synergistic manner.
The inferior part rotates the scapula by pulling the lower end of the scapula laterally and forward.
When the shoulder girdle is fixed, all three parts can act to lift the ribs as in case of labored breathing to assist in respiration.
Because it is largely responsible for the protractio[bringing scapula forward and around rib cage as in punching], serratus anterior is also called Boxer’s muscle.
Acting in synergy with trapezius fibers, the serratus anterior also functions to rotate the scapula upward such as when lifting weight overhead.
Subclavius
The subclavius is a small muscle, located immediately below the clavicle. This muscle runs horizontally
It takes origin from the junction of the 1st rib and its costal cartilage and inserts into the inferior surface of the middle third of the clavicle.
It functions to depress the clavicle.
It is supplied by the nerve to subclavius.
Clinical Significance
Injury
Tears of the muscles of the pectoral region are rare. Pectoralis major injury may be seen in athletes, sportspersons who participate in high contact sports, powerlifters.
Poland syndrome
Poland syndrome is a congenital anomaly where there is deficiency of pectoralis major on one side of the body along with other manifestations like finger shortening, syndactyly, and hypoplasia of the hand.
Winging of the Scapula
Because serratus anterior functions to hold the scapula against the ribcage, a loss of function results in a specific clinical sign called winging due to protrusion of the scapula backwards.

The long thoracic nerve can get injured traction injuries or surgery of the region.
Traction injuries are the ones where the upper limb gets violently stretched in an injury.