Last Updated on July 30, 2019
Wrist x-rays are commonly done for wrist injuries and other wrist ailments.
Wrist x-rays are only able to tell about the status of
- carpal bones
- radiocarpal joint
- Carpometacarpal joint
- Distal radius
- Ulna
In clinical practice, the common x-ray views of the wrist are posteroanterior and lateral.
Oblique radiographs are included to increase sensitivity to carpal, metacarpal, and phalangeal fractures.
PA, lateral and the semipronated oblique views are part of the three-view wrist series. It is most commonly done wrist series.
If we add semisupinated oblique, also called reverse oblique, it is called four-view series.
Apart from wrist series special views can also be done as needed
[Read more about the anatomy of wrist]
Wrist Series Views

Posteroanterior or PA View
This view is interchangeably referred to as AP view though it is performed PA. It is also called palmar dorsal view.
The patient sits alongside the table.
With the shoulder, elbow and wrist at the same height [makes radius and ulna parallel], the affected arm is flexed at 90 degrees at elbow and wrist is rested on the table with the palm facing down on the image receptor
This view demonstrates the carpal joint spaces more clearly.
A good PA view has only minor superimposition of the metacarpal bases and the distal radioulnar joint has no or little superimposition.
Oblique Views
There are two oblique views. one is in semipronated position and other is in semisupinated position.
The semipronated oblique is useful in identifying scaphoid fractures, triquetrum and hamate injuries.
The reverse oblique is quite useful for detecting fractures of the ulnar-sided carpal bones
Lateral View
This x-ray is done at a right angle to PA view and shows multiple carpal bones. It allows the assessment of the alignment of the radius, lunate, and capitate when a dislocation is suspected.
It can be done traditionally where the patient keeps the forearm in neutral rotation. This demands to move the forearm to the desired position. However in horizontal beam lateral wrist projection, the movement of the limb is not required and instead, the projection is made horizontal instead of vertical
Special Views
Ulnar and Radial Deviation Views
Changes in the width of the intercarpal joint spaces may occur because of increased intercarpal mobility and the findings are better demonstrated in these views. In short, these views can provide information on the integrity of the carpal ligament system.
Flexion and Extension Views
These views are taken in positions of flexion and extension of the wrist. These again are helpful in evaluating carpal instability.
Clenched Fist PA views
Useful additional view for evaluating suspected intercarpal ligament damage. Widening of the joint space (>2 mm) is considered significant.
it is especially useful in scapholunate dissociation.
Carpal Tunnel View
The carpal tunnel view is an axial projection to look for medial and lateral prominences and the concavity. It is especially helpful to look for injuries of the hook of hamate, pisiform, and trapezium.
The patient sits or stands with the back facing the table and palmar surface of hand is placed in contact with the cassette placed at the table margin.
The wrist is dorsiflexed approximately 135 degrees lifting the carpals and metacarpals away from the cassette. The best method to do this is to ask the patient to pull their fingers back with the other hand.
The resulting image provides a There should be a clear outline of the ventral aspect of the carpal bones.
Carpal Bridge View
The carpal bridge view is used to assess the dorsal aspect of the scaphoid, lunate and the triquetrum.
The patient sits along the table and dorsal aspect the wrist is placed on the cassette and wrist is flexed, as much as tolerable to the patient.
The x-ray provides, a clear outline of the dorsal aspect of the carpal bones with no superimposition.
This x-ray can be very helpful in imaging triquetrum fractures.
How to Visualize Wrist X-ray
For understanding the wrist x-ray, one needs to know how does a normal wrist x-ray look like.
Beginning proximally, the following structures are looked at as we move distally on x-ray.
- Distal radius
- Distal ulna
- Carpal bones
- Alignment
- Metacarpals
Distal radius
- AP view
- Distal radial articular surface should cup the carpals
- Radial styloid is the most distal portion of the articular surface
- Lateral view
- Radial surface should be smooth
- Distal radial cortical irregularity or a lucent line [fracture]
- Look for an ulnar styloid avulsion or intra-articular extension.
Check the ulna styloid
- Look for structural integrity and presence of a fracture line
- Note for any radiolucent lesion
Ulnar Styloid
- However, trace the cortex of the ulna
- Look for any avulsion
Carpals
There are eight carpal bones
These are scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate and hamate.
In the following x-ray, each carpal bone has been marked.
The carpus has eight bones in two rows
The proximal row consists of the scaphoid, the lunate, and the triquetrum.
The distal row consists of Trapezium, trapezoid, capitate, and hamate.

In the x-ray, the bones have been marked as follows.
S – Scaphoid
L- Lunate
T – Triquetrum
P – Pisiform
Tm – Trapezium
Td – Trapezoid
C – Capitate
H – Hamate
The most commonly injured carpal bone is the scaphoid. It is also important because of the risk of avascular necrosis.
- Look at the cortex of the scaphoid on all views
- Trace the cortices of the other carpal bones.
Alignment
On the lateral view, a line drawn through the distal radius, lunate and capitate should be smooth.
The lunate should sit within the cup of the distal radius.
The capitate should sit in the cup of the lunate
Any disruption of the line must raise suspicion of carpal dislocation
Carpal arcs [Gilula arcs]
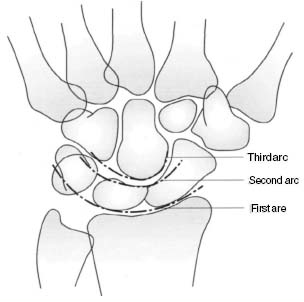
Articular surfaces of the carpal rows form three smooth lines. Tracing these arcs in a normal x-ray, PA view, will reveal 1-2 mm joint space between the carpal bones.
A widening of the space between the scaphoid and lunate is seen in scapholunate dissociation.
Distally, the joint space between the distal carpal row and the metacarpals is visible all along. If there is an overlap it carpometacarpal dislocation.
Metacarpals
Trace the base of each metacarpal for continuity. Look for any lesion or fracture line. Small avulsion fracture need to be looked very carefully.