Last Updated on November 20, 2019
Patellofemoral pain syndrome is characterized by pain or discomfort in the anterior aspect of knee anterior knee pain involving the patella and retinaculum which is not attributable to any intra-articular and peri-patellar pathology.
Sportspersons who put heavy stress on their knees like runners, jumpers, skiers, cyclists and football players are often vulnerable to this condition.
It frequently also occurs in manual laborers.
Patellofemoral pain syndrome forms a group of conditions referred to as runner’s knee. Other conditions include patellofemoral malalignment and chondromalacia patella.
Chondromalacia patellae is a term sometimes considered synonymous with patellofemoral pain syndrome but patellofemoral pain syndrome is a term that applies only to individuals without cartilage damage [chondromalacia patellae is the condition characterized by softening of the patellar articular cartilage]
Relevant Anatomy
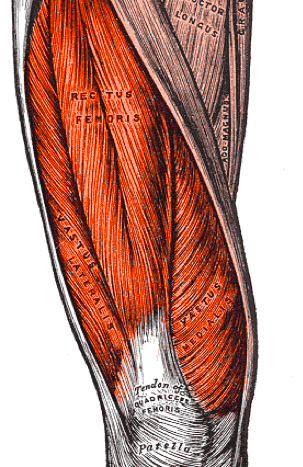
The patella is the kneecap bone and can be palpated easily on the anterior aspect of the knee. The patella bone lies within the quadriceps tendon. Quadriceps muscle consists of four heads namely vastus medialis which is on the medial aspect of the femur, vastus lateralis which is on lateral aspect, vastus intermedius which is in between and rectus femoris which is on anterior aspect femur and overlies intermedius.
The quadriceps tendon inserts on to the patella from which patellar tendon inserts on the tibial tuberosity.
The quadriceps muscle is powerful extensors and straightens the leg at the knee joint.
The back of the patella is covered with smooth cartilage. This helps the patella to glide over the lower part of the thigh bone at the time of the motion.
Causes of Patellofemoral Pain Syndrome
Patellofemoral pain syndrome is caused by various factors which put a strain on knee joint and on the surrounding muscles and ligaments. This can be due to overuse of the knee due to increased levels of physical activity [as in increased training], malalignment of the patella when it moves in the groove, muscle imbalance and tight retinaculum or iliotibial band.
Malalignment and overuse may be the most common reason for getting patellofemoral pain.
Flat foot makes the foot roll inwards and the knee has to compensate for the inward movement. Similarly, hard shoe soles put more strain on the knee. Repeated knee injury or joint hypermobility can also contribute
Fractures, internal knee derangement, osteoarthritis of the knee and bony tumors in or around the knee are secondary causes of patellofemoral pain syndrome.
Clinical Presentation of Patellofemoral Pain Syndrome [Signs and Symptoms]
The onset of the condition is usually gradual and initially intermittent, although some cases may appear suddenly following trauma.
Knee pain is the most common symptom and the pain is vague around patella [knee cap]. It could be localized behind the kneecap also. The patient, when asked for the location of the pain often place a hand over the anterior patella or describe a circle around the patella (circle sign).
Activities that load the knee extensor mechanism like climbing up and down the stairs, squatting, cycling or running may initiate and worsen the pain.
Prolonged sitting with bent knees would also cause the pain [Movie sign or theatre sign – because individuals might experience pain during prolonged sitting to watch a film or similar activity]. Apart from pain, crepitus in the joint due to rubbing of bones or giving way of the knee may be reported.
Swelling is usually minimal and the presence of the swelling should alert the physician to rule out underlying pathology.
On physical examination, tenderness often is present along the facets of the patella [Facets are depressions on the posterior aspect of the patella separated by a vertical ridge]. The facets are most accessible to palpation by manipulation of the patella while the knee is fully extended and the quadriceps muscle is relaxed. Manual positioning of the patella medially, laterally, superiorly, and inferiorly allows for palpation of the respective facets.
Repetitive squatting may reproduce knee pain.
Examination of the other limb is important, as the syndrome often is bilateral. However, one side usually manifests more symptoms.
Tenderness of tibial tuberosity may suggest that other impairments also are present.
Genu recurvatum and hamstring weakness may contribute to the occurrence of patellofemoral pain syndrome
Lab Studies
Laboratory studies generally are not indicated for the diagnosis of patellofemoral pain syndrome.
Imaging
Imaging studies usually are not necessary for diagnosis or treatment for patellofemoral pain syndrome but should be considered for unusual presentations and when the patient does not respond to treatment.
Anteroposterior, lateral and skyline views are desirable.
Xrays may show lateral patellar tilt and a high-riding patella (patella alta), osteophytes or joint space narrowing may in cases of osteoarthritis.
Computed tomography scanning and magnetic resonance imaging allow for imaging at various angles of flexion and identify malalignment using CT scanning.
MRI may give more insight into diagnosis and treatment when the presentation is uncommon or there is treatment failure.
Arthroscopy helps to confirm the diagnosis of patellofemoral pain syndrome by allowing direct visualization of the cartilage surface and assessment of joint structures that may cause symptoms similar to patellofemoral pain syndrome.
Differential Diagnoses
- Patellar tendonitis
- Prepatellar bursitis
- Plica syndrome
- Sinding Larsen Johansson syndrome
- Osgood Schlatter disease
- Patellofemoral arthritis
Treatment of Patellofemoral Pain Syndrome
In an acute episode, RICE treatment is given
- Rest [knee activity should be reduced until the pain is resolved. For pain originating from sitting too long, straightening the leg or walking is adviced]
- Ice application for 15 minutes in a go repeated over time.
- Compression
- Elevation should be used
NSAIDs may be used to relieve pain.
All the activities that cause knee pain should be stopped and the patient is put on physical therapy which consists of exercises aiming at the restoration of muscle balance of quadriceps, improving range of motion, and restricting the offending activity.
Strengthened quadriceps muscle helps to stabilize the patella.
Patellar taping, proper footwear and foot orthoses [to bring subtalar nearly neutral position] and knee bracing are adjuncts that help to reduce pain and improve function.
In long-term, the patient is instructed to modify activities that require loading on knee e.g. squatting
Surgical intervention is indicated rarely. Surgical procedures performed for patellofemoral arthritis include lateral facetectomy and patellar resurfacing.
Arthroscopic drilling of osteochondral defects allows healing of the defect with fibrocartilage and makes the symptoms better
Prevention
Staying in shape, stretching and flexibility exercises, training carefully and using proper running gear, avoid sitting, squatting, or kneeling in the bent-knee position for long periods of time can help to prevent patellofemoral pain syndrome.
Prognosis
The prognosis for full functional recovery is very good. In general, this syndrome is successfully treated with conservative measures.