Last Updated on October 24, 2021
Plantar fasciitis is a common cause of heel pain and occurs due to degenerative changes at the insertion of the plantar fascia on calcaneal tuberosity. The plantar fascia is the most common cause of heel pain for which professional help is sought.
A heel spur is commonly found in plantar fasciitis patients, but many asymptomatic persons also have heel spurs.
Plantar fasciitis could be bilateral in almost one-third of cases. It is usually seen in people aged 40-60 years. Early incidence is noted in people with spondyloarthropathies.
What is Plantar Fascia?
The plantar fascia is fibrous aponeurosis which originates from the medial tubercle of the calcaneum and runs forwards and inserts on short transverse ligaments of the metatarsal heads. It further divides into 5 digital slips and forms the fibrous flexor sheaths on the plantar aspect of the toes.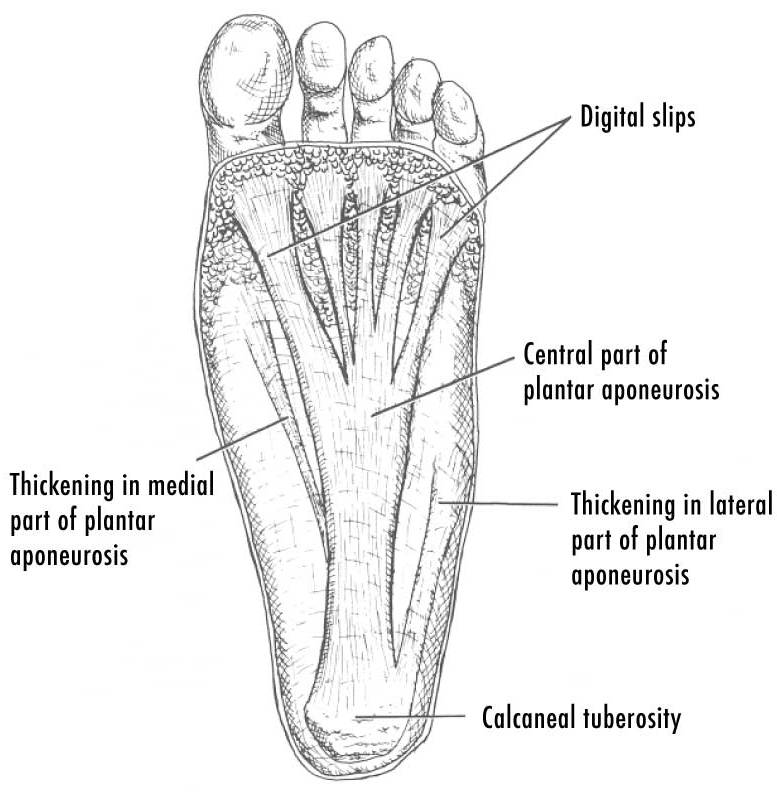
The plantar fascia is made up of the medial band, central band, and the lateral band.
The central part is the strongest section, and most commonly is involved in plantar fasciitis.
Plantar fascia supports the foot arches and acts as a tension bridge providing static support and dynamic shock absorption.
How Does Plantar Fasciitis Occur
The most common causes of plantar fasciitis are biomechanical dysfunction of the foot with overuse. Malignancies, arthritic changes, trauma, and infections may be other causes.
When the plantar fascia is stretched excessively, causes microtrauma along its course or at insertion on calcaneum. Repeated microtrauma leads to degeneration of fibers of the fascia.
Because inflammatory changes are not always present, the disease is thought to be a degenerative process characterized by an increase in the size of fibroblasts, disorganized collagen, and haphazard increase in vascular tissue with zones of avascularity – term suggested now is fascists instead of fascists.
The exact cause of plantar fasciitis is not clear. Multiple factors are thought to play a role.
There are two kinds of risk factors associated with plantar fasciitis.
- Extrinsic – which include training errors and equipment
- Intrinsic which could be related to the structure and function of the foot
Extrinsic risk factors
- Training related [most common cause]
- Increase in the distance
- Increase in intensity of training – speed workouts
- Increase in duration, or duration of activity
- Change of training surface – running on hills or uneven surface
- Ill-fitting or ill cushioned footwear
Intrinsic Risk Factors
Intrinsic factors lead to altered biomechanics and increased stress on the plantar fascia. Known intrinsic factors are
- Flat foot
- Overpronation of foot
- High arched foot
- Leg -length inequality
- Excessive lateral tibial torsion
- Excessive femoral anteversion.
- Tightness in the calf muscles and Achilles tendon
- Weakness of calf or foot muscles
- Degenerative changes in the heel or heel fat pad atrophy
Presentation of Plantar Fasciitis [Signs and Symptoms]
Pain is the primary complaint and it is mainly felt on the plantar surface of the foot in the heel region. Radiation to other parts may be noted in severe cases. Most of the patients report the pain to be severe in the morning after the first few steps. [After prolonged inactivity, such as sleeping or sitting]
The patient may limp and walk on his toes.
In the early stages of the disease, pain decreases with ambulation or warm up, but may increase during the day due to greater activity.
Tightness in the foot may be a complain. Patients in ja ob that require prolonged standing have symptoms worsened by the end of the day
There could be a history of increased activity prior to the onset of the pain like running or walking. A history of change of running surface, change in footwear may have occurred before the pain started.
If there is a night time pain, systemic symptoms like fever or presence of paresthesia points to causes other than plantar fasciitis.
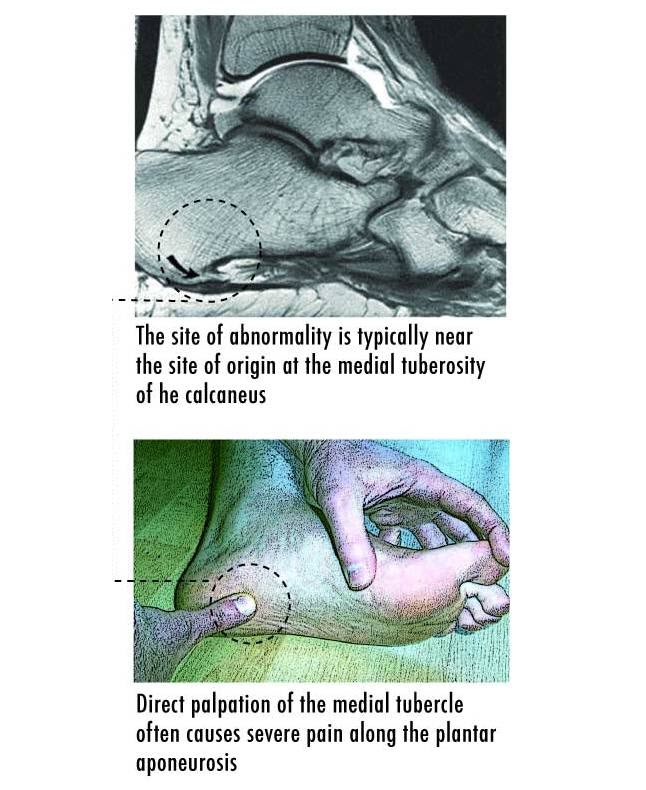
On examination, there may be tenderness in plantar-medial calcaneal tubercle and pressing it reproduces the pain.
Toe walking and dorsiflexion of the toes may reproduce the pain. [The latter is also called the windlass test]. A tight Achilles tendon is a common finding. The patient should be examined to rule out intrinsic factors.
Tenderness on the posterior aspect of the heel and ankle suggests retrocalcaneal bursitis or Achilles tendonitis.
Patient should be examined to rule out other possible ailments [See differentials]
Diagnostic Considerations
- Calcaneal stress fracture
- Calcaneus bone injuries
- Paget disease
- Tumor
- Achilles Tendonitis
- Contusions
- Lumbosacral Radiculopathy
- Retrocalcaneal Bursitis
- Tarsal Tunnel Syndrome
- Plantar fascia rupture
- Neuropathic pain
- Spondyloarthropathies
Lab Studies
Lab studies are generally not required for diagnosis but may be used to investigate other causes of heel pain if suspected. Complete blood count, erythrocyte sedimentation rate, metabolic panel, and rapid plasma reagin [RPR] and rheumatoid factor can be done to rule out common pathologies.
Imaging
Radiographs typically are not necessary for diagnosing plantar fasciitis but are don to rule out conditions like ba one tumor or fracture.
Lateral heel x-ray may reveal a plantar heel spur and is an indicator of chronic across the plantar fascia for at least 6 months. Many patients with plantar fasciitis have no heel spur.
The spur is as a result of the stresses and per se not the causation.
MRI is rarely done and confirm or rule out fasciitis. It also helps to diagnose plantar fascia rupture. Plantar fascia thickening and surrounding edema can also be detected on MRI.
Ultrasonography is rarely used and can reveal an increase in the thickness of the fascia edema of the fascia where it inserts into the calcaneus.
Bone scan is not routinely needed and is helpful for patients in whom stress fracture of calcaneum is suspected and shows shows increased uptake over the medial calcaneal tuberosity. In stress fracture, the increased uptake is somewhere else in the calcaneum.
CT is also used to confirm a stress fracture if there is a strong suspicion.
Electromyography is useful to analyzing neurologic entrapment syndromes.
Treatment
Up to 90% of patients respond to non operative treatment. These treatments include rest and activity modification, ice therapy, drugs, splinting, and orthoses.
The treatments should be used in combination for better success..
These treatment options should be tried for 6 weeks. Those cases which do not respond by that time should be considered for a local injection. Recalcitrant cases should be considered for surgery.
Ice Therapy
Ice therapy is the first line of treatment for plantar fasciitis especially in athletes. Ice should be applied daily . It can be applied after completing stretching, and strengthening exercises.
Rest
Rest is an essential part of the treatment of plantar fasciitis. This could be achieved by modification of activity or relative rest.
In patients with severe pain, a period of casting or immobilization may be required.
Athletes must modify activities such as decreasing the amount, frequency, or intensity of the activity.
Other Measures
Improper footwear must be replaced by a better one. A worn out shoe should be replaced by a new one.
Persons with flat feet and overpronation can use motion control shoes. A motion control shoe has the Rollbar technology combined with the medial and lateral posts. If your shoe wears out at the inner tread near the ball of the foot, you might need motion control shoe. Motion control shoe typically feature a straight-lasted, board-lasted, or combination-lasted construction; an external heel counter; a wider flare; and extra medial support.
[For more on Shoe anatomy, please visit AAPSM ]
Runners with high arched shoes should wear with greater cushion.
Drugs
NSAIDs are useful pain relievers. Oral corticosteroid can be used in acute phase of plantar fasciitis.
Local Injections
Local corticosteroid injections are generally applied after primary conservative treatment has failed. The results are better with ultrasound guided injections than palpation-guided method. Triamcinolone and betamethasone sodium are frequently used steroids for injections..
Injections of botulinum toxin type A have been shown to bring improvements in pain relief and overall foot function.
Autologous blood injection into the plantar fasciais thought to stimulate the healing process by inducing inflammatory reaction and few studies have provided the evidence it could be beneficial in the treatment of chronic plantar fasciitis.
Extracorporeal shock-wave therapy sends high-pressure sound waves to stimulate blood flow, reinjure tissue to stimulate healing, andshut down the neuronal pain pathways.
Splints
Night splints
Night splints maintain 90 degrees foot leg angle and do not allow natural plantar flexion of the feet. Most of the people sleep with feet plantar flexed and this causes the plantar fascia to be shortened in plantar fasciitis patients. This is the reason pain is worse in the morning on taking first few steps. Night splints thus constantly cause passive stretching of the Achilles tendon and plantar fascia.
Orthoses and Shoe Modifications
Patient should wear a shoe with a supportive heel counter and stiff midsole and Fashionable shoe wear often does not provide sufficient support for the arch and further exacerbates the problem. In general, lace-up shoe gear is recommended to maximize support. In one study, 14% of patients credited the change in shoe gear as the best treatment.
Shoe inserts or taping can help to relieve the symptoms in low arched feet.
Custom orthotic devices can be individualized for flat feet, heel valgus and leg length inequality.
Exercises for Plantar Fasciitis
Initially, stretching exercises of calf and foot are done. These include wall stretches, towel stretch and stair stretch.
Passive dorsiflexion on the toes with simultaneous stretching of the Achilles tendon has been found to be especially useful.
Following stretch exercise, strengthening exercises like towel curls, marble (or coin) pickups, and toe taps.
Towel curl
The patient sits on the chair with the affected foot lying flat on the end of a towel that is placed floor. The patient using his toes curls up the towel to pull it towards him while keeping the heel on the floor. As Weight may be added to the far end of the towel to increase the difficulty when aility of the patient increases.
Marble Pickups
Marbles are placed on the floor near a cup and patient picks them up with his toes and drops them in the cup while keeping the heel on the floor. Difficulty can be increased by replacing marbles with coins.
Toe Taps
The patient lifts all the toes off the floor and heel is kept on the floor. First, the floor is tapped with big toe while other 4 toes are kept in the air. Next, the big toe is kept in the air and other four toes are tapped.
Stretching or strengthening exercises should continue about 2-3 times per week.
[Read more on Exercises for Plantar Fasciitis]
Surgery For Plantar Faciitis
Surgical treatment may be required in In 5-10% of cases of plantar fasciitis. Surgery is indicated in patients where 6-12 months of conservative treatment has failed.
The surgery involves release by sectioning part or all of the fascia via an open or endoscopic procedure. Overall, surgical release has a 70-90% success rate in treating patients with this condition
Instability of the medial column, flattening of the longitudinal arch and heel hypoesthesia are the potential side effects.
Percutaneous partial fasciotomy, cryosurgery, bipolar radiofrequency microdebridement are newer procedures which are being tried and show promising results
Complications
In rare cases, the plantar fascia may rupture spontaneously. The risk of such a rupture is greatly increased by a history of treatment with a corticosteroid injection. Corticosteroid injection into the superficial fat pad may cause fat pad necrosis.
Untreated plantar fasciitis may become a chronic condition. Knee, hip and back problems may develop.
Prognosis
About 80% of plantar fasciitis cases resolve spontaneously by one year. About 5% of patients end up undergoing surgery for plantar fascia release.
Progressive plantar pain, limping, and restriction of activities may occur in an untreated plantar fasciitis.
Prevention of Plantar Fasciitis
Following points should be taken care of in athletes with plantar fasciitis
- Proper warm up and stretch before activity
- Icing after activity.
- Wear appropriate shoes
- Change shoes y 250-500
- Adequate padding, proper sole stiffness, and appropriate arch support all can help