Last Updated on October 29, 2023
Poland Syndrome is a congenital condition characterized by the absence of chest wall muscles on one side of the body and short, webbed fingers of the limb of the same side.
The Poland syndrome is also known as Poland Anomaly, Poland Sequence, and Poland Syndactyly.
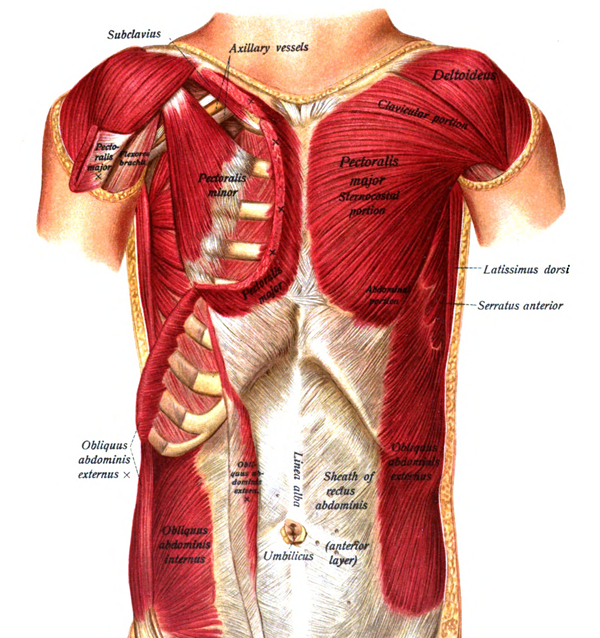
Relevant Anatomy
The pectoralis major is a large muscle of the upper chest wall which gives the chest its shape and forms the anterior edge of the axilla. It arises from sternum or breastbone, clavicle and cartilages of the second to the sixth ribs. It inserts on to shoulder and is particularly useful in pushing and rowing activities.
Pectoralis minor is underneath pectoralis major arises from the third to fifth ribs and functions to rotate the shoulder.
Poland syndrome, named after British surgeon Alfred Poland.
Males are more commonly affected than females. The right side is more affected than left.
The exact incidence of the disease is not known.
Most Poland syndrome cases arise sporadically.
However, familial involvement has been reported, suggesting some degree of genetic transmission.
Association with Mobius syndrome and Klippel-Feil syndrome is known. Malignancies like leukemia and non-Hodgkin lymphoma, may occur in patients with Poland syndrome.
Features of Poland Syndrome
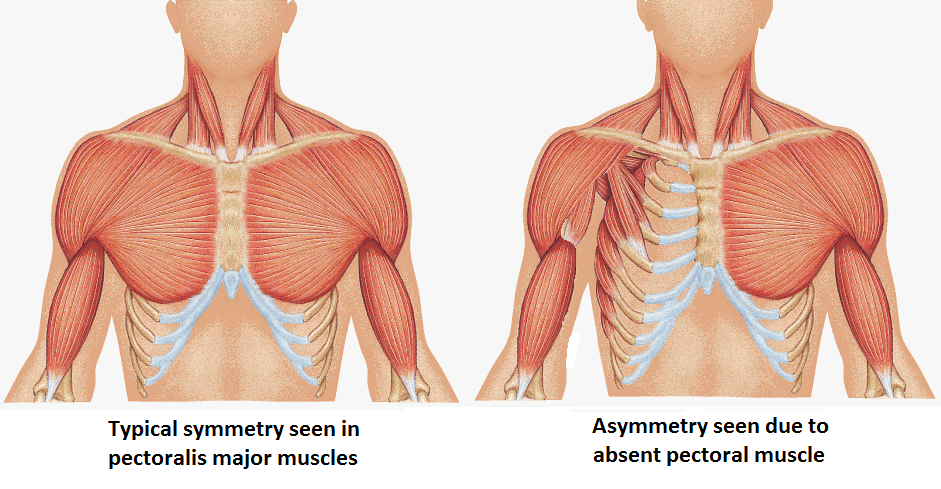
There is the absence of the pectoralis minor on one side and the sternal part of the pectoralis major muscle.
The absence of the sternal head of the pectoralis major muscle is considered the minimal expression of this syndrome.
Other muscles which can be involved are the pectoralis minor, serratus, latissimus dorsi, and external oblique muscle.
Other variable associated features are
- Underdevelopment or absent nipple and areola
- Nipple higher than the normal nipple
- Absent of axillary hair
- Hypoplastic of breast and underlying tissues in females
- Skeletal abnormalities
- Underdevelopment or absence of upper ribs
- Elevation of the shoulder blade (Sprengel deformity)
- Shortening of the arm
- Underdevelopment of the forearm bones
Causes of Poland Syndrome
Exact cause of Poland syndrome is not known.
Majority of cases appear to occur sporadically but rare familial patterns have been observed.
Early interruption of blood flow due to to the subclavian artery supply disruption has been suggested the initiating event. More proximal the occlusion, severer are the symptoms.
Depending upon the location and severity of involvement, the clinical presentation may of Poland Syndrome, Mobius Syndrome, Klippel-Feil Syndrome, and Sprengel deformity.
That is why Poland Syndrome is sometimes referred to as Poland sequence. [A sequence refers to a pattern of malformations derived from a single anomaly.]
Related Disorders or Sequences
Mobius Syndrome
Poland Syndrome has been reported to occur in association with Mobius Syndrome, known as Poland-Mobius Syndrome.
These patients are characterized by facial paralysis due to paralysis of the sixth and seventh cranial nerves (Mobius Syndrome) and features typically seen in Poland Syndrome.
Masklike expressionless face, drooped eyelids, tongue hypoplasia, poor suckling and swallowing, speech impairment and mental retardation are seen.
Charlie M Syndrome
It is a rare condition characterized by certain distinctive facial and limb malformations.
The syndrome is characterized by
- Widely spaced eyes or ocular hypertelorism
- Broad nose and small mouth
- Cleft palate
- Micrognathia – small jaw
- Facial nerve paralysis in some cases
- Absent or cone-shaped front incisors
- Asymmetric abnormalities of the fingers and toes
Clinical Presentation of Poland Syndrome
The right side is more commonly involved. The patient would have obvious chest asymmetry and deformity.
The affected side would have absent nipple and areola with minimum subcutaneous fat. Tasymmetryery may be pronounced by rib cage abnormalities. The affected limb has short arm or forearm or both. There would the be the absence of the sternal head of the pectoralis major muscle.
The patient would have short joined fingers or brachysymphalangism.
Associated muscles which could be underdeveloped or absent are serratus, external oblique, pectoralis minor, latissimus dorsi, infraspinatus, and supraspinatus muscles. There could be a total absence of anterolateral ribs or lung herniation on the affected side.
Though Poland syndrome is present at birth, most of the patients do not seek consultation till late for aesthetic reasons.
The examination is carried out to know the status of following for purpose of treatment.
- Stage of breast development
- Status of the latissimus dorsi muscle – Present or absent or hypoplastic
- Extraocular movements – to look for associated Mobius syndrome.
- Abnormal elevation and/or underdevelopment of the scapula
- Sprengel Shoulder
Investigations
CT scan is done to determine the extent to which the muscles and bones of the chest wall are affected.
CBC and blood film examination are done when leukemia and non-Hodgkin lymphoma is suspected.
Treatment of Poland Syndrome
Many patients may not seek he treatment. The treatment of Poland Syndrome would depend on the specific symptoms.
Generally, the patients present for treatment of the chest deformity and breast asymmetry. Some patient may not want surgical treatment and counseling would suffice.
Following are important determinants that influence the timing and options for reconstruction:
- Gender
- Breast development
- Presence of latissimus dorsi muscle,
- The degree of chest wall deformity.
Male Patients
Chest deformity can be reconstructed with the latissimus dorsi muscle as early as age 13 years. Rib abnormalities if severe, need to be addressed.
Female Patients
Breast reconstruction provides the best results once the breast has fully developed.
Before that, one may consider early treatment with a temporary expander especially if the patient is psychologically being affected.
[Breast implants and expander should not be placed in patients who are too young.]
Upon completion of breast development (18-19 years of age), the tissue expander can be removed and the breast can be reconstructed with the latissimus muscle transposed over a permanent implant.
If the latissimus is absent, opposite latissimus dorsi or other adjoining muscles may be tried.
Sometimes, therapeutic tattooing is used to compensate for a missing nipple.