Last Updated on October 19, 2019
A pulled muscle in chest means a tear or injury in the muscles of the thoracic cage.
Relevant Anatomy
Thoracic cage is composedof 12 pairs of ribs and sternum.
{read more about thoracic cage anatomy}
The muscles of the thoracic cage are
- Intercostals
- External
- Internal
- Innermost
- Subcostals
- Transversus thoracis
All of these muscles act to change the volume of the thoracic cavity during respiration. That is why a pulled muscle in chest pains with breathing, sneezing or coughing because these movements put a strain on these muscles.
Thought the term chest muscles also include other muscles, these are not considered here. These muscles do not comprise the thoracic wall but do attach to it. These include the pectoralis major, minor, serratus anterior and the scalene muscles What we normally refer as pulled chest muscles are the muscles of the thoracic cage..
Intercostals
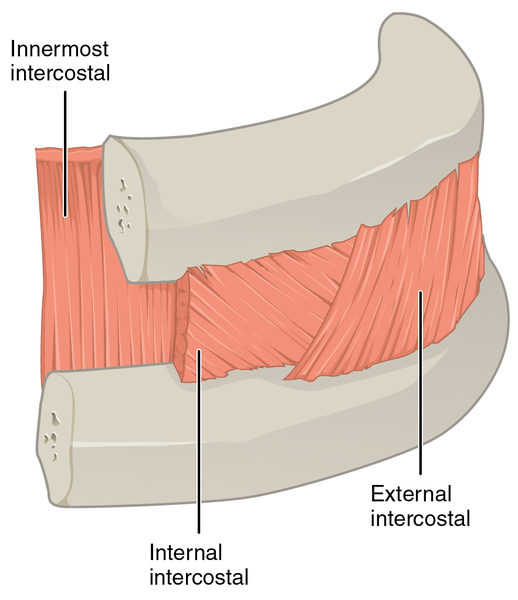
Image Credit: Wikipedia
The intercostal muscles lie in the intercostal spaces between ribs. They are arranged into three layers.
External Intercostals
There 11 pairs muscles. They run inferoanteriorly from the rib above to the rib below and are continuous with the external oblique of the abdomen.
These originate at the lower border of the riba and insert it into the superior border of the rib below.
External intercostals elevate the ribs, increasing the thoracic volume.
These are supplied by intercostal nerves T1-T11.
Internal Intercostals
These lie deep to the external intercostals. These originate from the lateral edge of the costal groove, directed anteroposteriorly and inserts into the superior surface of the rib below.
Internal intercostals are continuous with the internal oblique muscle of the abdominal wall.
The muscles that attach to bony rib reduce the thoracic volume by depressing the ribcage whereas those which are between the cartilaginous part of the ribs elevate the ribs.
These muscles are supplied by intercostal nerves T1-T11.
Innermost Intercostals
These form the deepest layer of the intercostal muscles are the deepest of the intercostal muscles. These originate from the medial edge of the costal groove and insert into the superior surface of the rib below.
They are separated from the internal intercostals by the intercostal neurovascular bundle. These muscles and are in the most lateral portion of the intercostal spaces.
Their action is similar to internal intercostals and the nerve supply is similar too.
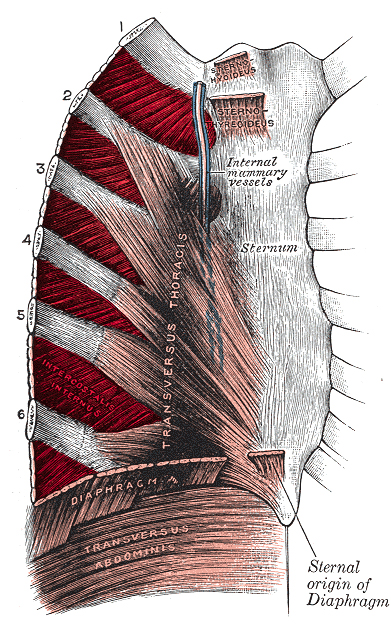
Transversus Thoracis
These muscles originate from the posterior surface of the inferior sternum to the internal surface of costal cartilages 2-6. The muscles are continuous with transversus abdominis inferiorly.
Transversus thoracis muscle acts as a weak depressor of the ribs.
The nerve supply is by intercostal nerves T2-T6.
Subcostals
The subcostal muscles are found in the inferior portion of the thoracic wall. These are thin slips of muscle, which originate near the angle of the rib and attach to the second and third ribs below. The direction of the fibers parallels that of the innermost intercostal. The actions and nerve supply is similar
Causes
Intercostal muscle strains are the most common cause of musculoskeletal chest pain.
Main causes of pulled chest muscle are
- Injuries due to overstretching, muscle fatigue and repetitive injuries
- Direct trauma by an object hitting
- Lifting heavyweight
- chronic poor posture
- Fall
- a severe cough
- Forceful sneeze
- Sports injuries
In sports stiffness of muscles and inadequate warm-ups may contribute.
Clinical Presentation and Diagnosis
A pulled chest muscle presents with an acute onset pain that is worsened by chest movements. The pain worsens with deep breathing, coughing or sneezing.
The pain is often localized to a region but could be diffuse in some cases like blunt trauma.
There would be a region of tenderness within the chest wall.
Most of the pulled chest muscles don not have an underlying lung or pleural injury, a risk in rib fracture.
Chest pain always raises a concern and because of the gravity of the diagnoses which could present as chest pain, the pulled muscle in a chest is sometimes a relief.
Still, the chest pain should be taken seriously and other causes of chest pain should be ruled out
- Heart attack
- Angina pectoris
- Pleuritis
The pain of pulled muscle in chest is not associated with any shortness of breath and other discomforts. Pain on movement of the chest such as twisting is typical of thoracic cage involvement.
The diagnosis is mostly clinical.
An x-ray chest is able to tell if the patient has a fracture of the rib or any underlying lung injury.
In most of the cases, the x-ray is normal.
No blood work is needed to reach a diagnosis.
Treatment
The treatment of pulled muscle consists of RICE therapy and medication.
RICE Therapy
RICE therapy consists of rest, ice application, compression, and elevation.
Rest
Rest to the injured muscle can be done by avoiding strenuous activities, or tasks which would lead to deep breathing.
Ice
Ice packs are applied over the pain site for 15-20 minutes in an hour several times a day. If ice packs are not available, ice can be wrapped in polythene or towel.
Compression
A clothe can provide compression when wrapped snuggly around the chest. Commerical chest binders are also available.
Elevation
This can be achieved by sitting and sleeping in a reclining position. Extra pillows can be used for support.
This position also protects from thoracic pressure being raised due to abdominal push when we lie down.
Drugs
Medication is mainly for pain relief. Nonsteroidal anti-inflammatory drugs usually are sufficient.
Muscle relaxants can be added if the pain is severe.
Cough suppressant medications are given if the patient has a cough.
When the pain becomes tolerable, deep breathing exercises are begun.
Most of the cases of a pulled muscle in chest recover within 1-3 weeks.