Last Updated on August 1, 2019
Sacral fractures are common in pelvic injuries and associated with 30-45% cases. About a quarter of sacral fractures are associated with neurologic injury. Sacral fractures are missed quite often, as often as 75% in patients without a neurological deficit and about half of those with the deficit.
Neurologic injury associated with sacral fractures can range from an incomplete injury of a single nerve root to involvement of the entire cauda equina. The injury can range from a neuropraxia to transection of nerve roots, or even complete transection of the cauda equina.
Sacral fractures either result from high energy trauma in young adults or occur as insufficiency fractures in the elderly as a result of low energy falls.
Sacral fractures are usually associated with pelvic fractures. The sacral fracture associated with lateral compression pelvic fractures is usually stable but sacral fractures associated with vertical shear pelvic fractures are usually unstable. Sacral fractures may involve injury to the lumbosacral junction and result in varying degrees of lumbosacral instability or even lumbosacral dissociation.
L5 nerve root runs on top of the sacral ala whereas S1-S4 nerve roots are transmitted through the sacral foramina. S2-S5 nerve roots perianal sensation and function to control anal sphincter tone and voluntary control. In addition, these function to maintain bulbocavernosus reflex.
Detailed anatomy of sacrum can be read here.
Classification of Sacral Fractures
Denis classification
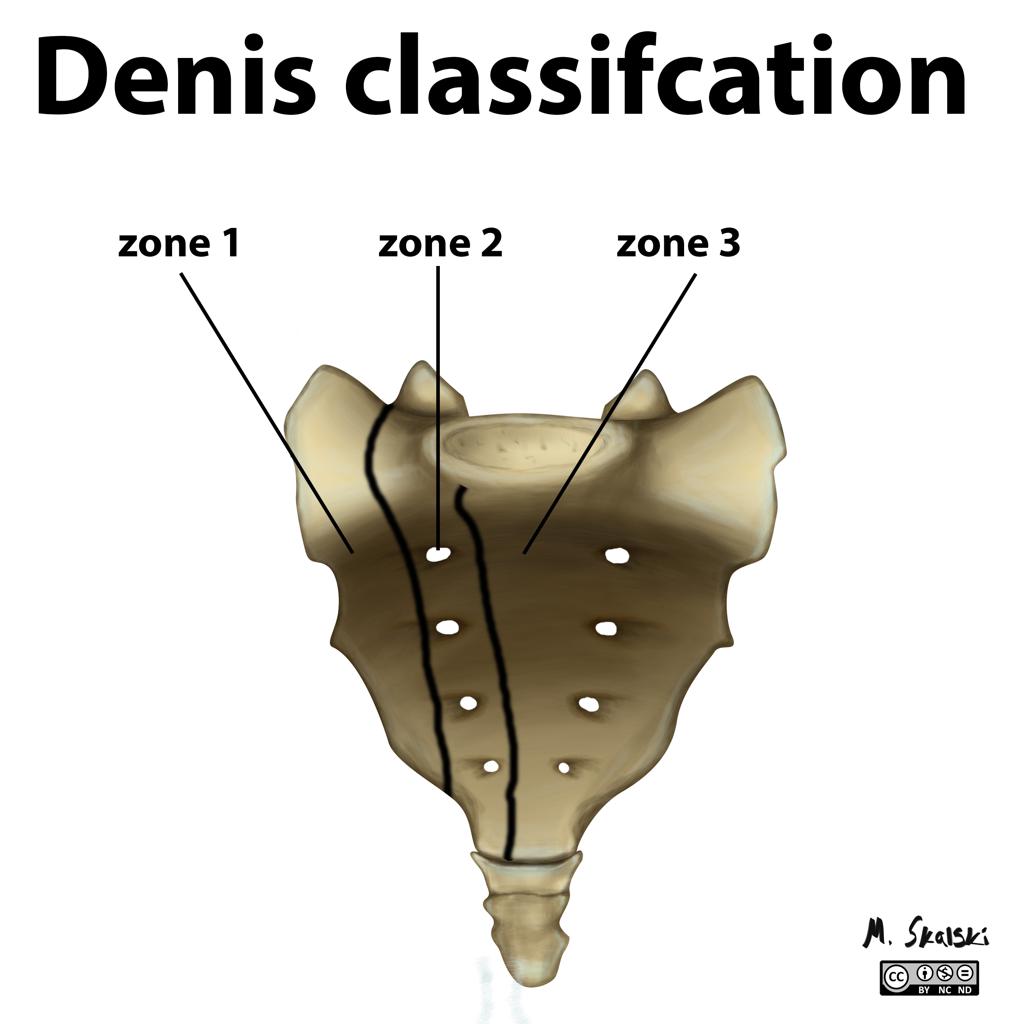
Zone 1
Zone 1 fractures are sacral fractures lateral to foramina. These are most common fractures and associated with the nerve injury in 5%. Usually, the L5 nerve root is affected.
Zone 2
These are the fractures through foramina. These fractures could be stable or unstable and are associated with an increased risk of nonunion and poor functional outcome
Zone 3
These fractures are medial to foramina and involve the spinal canal. These fractures have the highest rate of neurologic deficit [up to 60%] including bowel, bladder, and sexual dysfunction.
Transverse sacral fractures occur in <5% of sacral fractures. They are classified as Denis 3 as they traverse the spinal but the fracture line often traverses all 3 zones.
They have been further classified on morphological pattern H, U, lambda and T-shaped fractures.
Another classification is Roy-Camille/Strange-Vognsen and Lebech Classification of Transverse Sacral Fractures.
Type 1
There is a kyphotic angulation at the fracture.
Type 2
Fractures have both kyphosis and partial anterior translation.
Type 3
Fractures have kyphosis along with a complete translation.
Type 4
Fractures have segmental comminution of the S1 body due to axial compression
Isler Classification
This classification is of fractures involving the lumbosacral junction and is based on the location of the major fracture line on relation to the L5-S1 facet [which impacts the potential for lumbosacral instability.]
Type I
Fractures of the lumbosacral junction lateral to the facet. These generally do not affect lumbosacral stability. Pelvic ring stability may be affected.
Type II
Fractures of the lumbosacral junction that exit through the L5-S1 facet.
Type III
Fractures of the lumbosacral junction that exit medial to the facet. Type III fractures are usually associated with significant instability of the lumbosacral junction. Bilateral type III injuries may represent lumbosacral dissociation.
Presentation of Sacral Fractures
The patient is usually a case of high energy trauma [ motor vehicle accident or fall from height]. Elderly patients may present with sacral fractures after a simple fall.
There is a pain in the posterior aspect of the pelvis. A presence or suspicion of fracture of the pelvis should alert the examiner to look for sacral fractures. All the examination for pelvic fractures must be done. In elderly patients with insufficiency, fracture tenderness may be elicited on the sacrum.
Therefore clinical examination of patients sustaining sacral fractures requires more than the just routine examination of lower extremity sensory and motor function. An additional examination is required to identify injuries to the lower sacral plexus.
This includes
- Rectal exam
- Light touch and pinprick sensation along S2-S5 dermatomes
- Perianal wink
- Bulbocavernosus reflex
- Cremasteric reflexes
Distal pulses should be examined.
Imaging
Xrays are the first line of imaging but about one third are able to show the fractures
Recommended views are Pelvis AP, inlet and outlet views. Inlet view provides the best assessment of the sacral spinal canal and superior view of S1. Outlet view provides a true AP view of the sacrum.
In addition, lateral view of sacrum can provide more information on sacral fractures as well as a lumbosacral junction.
CT is the imaging choice to identify the fracture pattern better. Coronal and sagittal reconstruction enhances understanding.
MRI is recommended for assessment of neural deficit.
Treatment of Sacral Fractures
Nonoperative Treatment of Sacral Fractures
Most sacral fractures can be treated nonoperatively. To treat nonoperatively the fracture should be
- Undisplaced/stable
- Without a significant associated pelvic ring disruption
- Not involving the lumbosacral junction
- Without neurologic injury.
Nonoperative treatment involves limitation of weight bearing with a gradual increase, orthosis.
Operative Treatment
Surgical fixation of sacral fractures is indicated in
- Fractures with displacement>1 cm
- Soft tissue compromise
- Persistent pain after non-operative management
- Displacement of fracture after non-operative management
Decompression is also indicated in fractures with the neural deficit.
Sacral Fracture Fixation
Displaced or unstable sacral fractures are best treated by closed or open reduction and internal fixation. Following types of fixations are used. Neural decompression when needed, may be achieved indirectly by fracture reduction, or a laminectomy or foraminotomy.
- Percutaneous Iliosacral Screws – most commonly used
- Posterior Sacral Tension Band Fixation – Vertically unstable comminuted sacral fractures or patients with a dysmorphic sacrum
- Lumbopelvic Fixation – In sacral fractures with associated lumbosacral instability [Pedicle screws placed in L5 and or L4 that are connected to fixation placed into the ilium from posterior to anterior.]
- Triangular Osteosynthesis – Placement of pedicle screws in the lower lumbar and the posterior ilium in conjunction with iliosacral screws.
Complications of Sacral Fractures
- Venous thromboembolism due to immobility
- Iatrogenic nerve injury
- Malreduction