Last Updated on March 11, 2020
Scapulothoracic bursitis is inflammation of the scapulothoracic bursae present between the scapula and rib cage.
Symptomatic scapulothoracic bursitis is not very common.
Another similar but different term used is scapulothoracic crepitus [snapping scapula] and it is important to highlight the difference.
Scapulothoracic crepitus is referred to as thumping or popping sounds that occur with scapulothoracic motion. The crepitus could be due to bony lesions or soft tissue lesions like bursa.
Thus, scapulothoracic bursitis can be a reason for crepitus, but scapulothoracic crepitus can be due to the causes other than bursa too.
Anatomy of Scapulothoracic Bursa
The scapula is a thin flat bone that articulates with humerus to form shoulder joint or glenohumeral joint. In the normal position, the scapula is rotated anteriorly approximately 30 degrees with respect to the trunk and tilted forward about 20 degrees in the sagittal plane. This position is also called the plane of the scapula.
The stability of the scapula is provided by the surrounding muscles. These muscles can be divided functionally into
- Scapulothoracic muscles – responsible for scapulothoracic motion coordination
- Rotator cuff muscles- responsible for glenohumeral movements
- Scapulohumeral muscles- responsible for providing strength to the humerus bone
The scapula contributes to shoulder motion during elevation. The first 30 degrees of elevation is at the glenohumeral joint and the next 60 degrees of elevation is by an equal contribution of scapulothoracic and glenohumeral motion.
Therefore, there is approximately a 2:1 ratio of glenohumeral: scapulothoracic motion. This is known as normal scapulohumeral rhythm.
A disturbance of this rhythm is one of the possible causes of scapulothoracic bursitis.
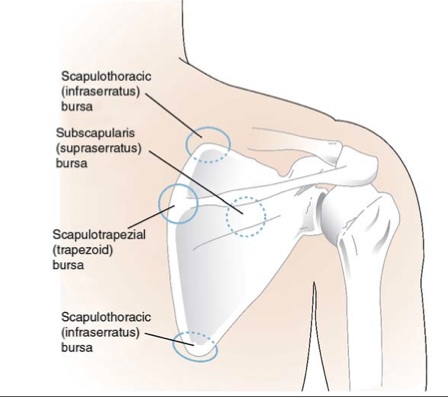
There are up to six scapulothoracic bursae present which allow for smooth, gliding scapulothoracic motion. These are
- Anatomic or major bursae
- Constant presence
- Infraserratus- between the serratus anterior muscle and the chest wall.
- Supraserratus bursa- between the subscapularis and serratus anterior muscles
- Adventitial or minor bursae
- Form as a response to abnormal biomechanics
- Two at the superomedial angle of the scapula
- One at the inferior angle of the scapula
- One trapezoid bursa- near the medial base of the spine of the scapula under the trapezius
Causes of Scapulothoracic Bursitis
Abnormalities of the bone or soft tissues can lead to scapulothoracic bursitis.
Bony abnormalities are the most common causes. Idiopathic causes are the next most common followed by resection of the rib
Each cause eventually disrupts the motion between the anterior surface of the scapula and the bony thorax.
A list of the causes is given below-
- Trauma – Fall on outstretched extremity causing injury to scapular soft tissues
- Overuse
- Often in sportspersons esp. overhead sports (eg, throwing, swimming, tennis)
- Professional work that requires repetitive scapular motion
- Osteochondroma – will cause crepitus earlier than bursitis
- Malunited fractures of rib or scapula
- Bone spurs
- Reactive bursitis to neighboring pathology
- Muscle fibrosis
- Muscle atrophy
- Anomalous muscle insertions
- Infections of bursa
Clinical Presentation of Scapulothoracic Bursitis
Pain in the scapular region which increases on activity of shoulder is the main complaint. There could be audible crepitus in some cases but crepitus due to subscapular bursitis is often soft.
A history of sports playing and other professional activities with repetitive motion of scapula may be sought.
On examination, there may be tenderness at the superomedial border and inferomedial border.
Adduction and internal rotation of the shoulder make scapula more prominent for palpation.
There may be winging of the scapula which suggests a space-occupying lesion in the scapulothoracic space. Scapular dyskinesis or disruption of normal scapulohumeral rhythm may be present.
Any crepitus present should be noted.
There could be increased scapular motion during elevation leading to protrusion at the lateral border of the axilla.
The posture of the patient needs to be observed for the forward head position as it may be contributory.
Lastly, neuromuscular examination should be performed which must include muscle testing of the following muscles
[read more on Shoulder Muscles]
- Trapezius
- Levator scapula
- Serratus anterior
- Latissimus dorsi
- Deltoids
- Rotator cuff muscles
Muscles should be examined for any stiffness too.
Diagnostic Workup
Injection of local anesthetic and corticosteroid may provide relief. This can be used to confirm the diagnosis as well as for treatment purposes of scapulothoracic bursitis.
X-rays may be normal or may show abnormalities of the bony origin. Anteroposterior view and a lateral view of the scapula are the usually ordered views.
CT scan is more helpful in the detailed analysis of the bony lesions. MRI, when done, is especially helpful in identifying the size and location of an inflamed bursa.
Electrodiagnostic studies can be sought to analyze muscle weakness or atrophy.
Differential Diagnosis
- Elastofibroma – benign connective tissue tumor
- Shoulder impingement
- Glenohumeral instability
Treatment
The initial treatment of scapulothoracic bursitis consists of
- Rest
- Nonsteroidal anti-inflammatory drugs for pain and inflammation control
- Curtailing and modifying the activity
- Heat
- Massage
- Ultrasound treatment
- Steroid injections into the lesion
- Shoulder rehabilitation exercises
Shoulder rehabilitation exercises have an important role in the treatment of scapulothoracic bursitis. These generally consist of
- Posture improvement
- Strength and endurance training of periscapular muscles
- Strengthening the periscapular muscles
- Endurance training consists of low-intensity exercises with high volume
- Core exercises
Patients who do not improve with nonoperative treatment may be considered for arthroscopic removal or bursa. The underlying cause of scapulothoracic bursitis needs to be addressed. This may warrant partial removal of the scapula.
References
- Carlson HL, Haig AJ, Stewart DC. Snapping scapula syndrome: three case reports and an analysis of the literature. Arch Phys Med Rehabil. 1997;78:506-511
- Kouvalchouk JF. Subscapular crepitus. Orthop Trans. 1985;9:587-588
- Manske RC, Reiman MP, Stovak ML. Nonoperative and operative management of snapping scapula. Am J Sports Med. 2004;32:1554-1565