Last Updated on April 6, 2022
The shaft of humerus fracture is the fracture of humerus bone that lies between the proximal and distal part of the humerus. This part lies between the upper border of the pectoralis major insertion proximally and the supracondylar ridge distally.
The shaft of the humerus constitutes the middle three-fifths of the entire humerus.

Relevant Anatomy

The shaft of humerus is cylindrical but distally humerus becomes triangular.
The intramedullary canal ends 2 to 3 cm proximal to the olecranon fossa.
Various muscles that take origin or insert at the shaft of the humerus are
[Read Muscles of the Arm]
- Deltoid
- Coracobrachialis
- Brachialis
- Triceps
- Brachioradialis
The deltoid tubercle forms a lateral prominence just proximal to the midshaft. The shaft of the humerus has a posterior, an anterolateral, and an anteromedial surface. The medullary canal of the humerus ends proximal to the olecranon fossa.
The arm is divided into anterior and posterior compartments by fascial septae. The posterior compartment contains the triceps muscle, and radial nerve between the long and lateral heads of the triceps.
The anterior or flexor compartment contains the flexors of the elbow, biceps brachii and brachialis, and the coracobrachialis. The brachialis has got two nerve supplies- one from the musculocutaneous and the other from the radial nerve.
The brachial artery and musculocutaneous and median nerves are present in the anterior compartment throughout the length of the arm.
The ulnar nerve takes origin from the anterior compartment but then passes into the posterior compartment in the distal arm. The radial nerve enters the posterior compartment proximally but comes to the anterior compartment in the distal portion.
The radial nerve arises in the axilla region and descends down the arm, traveling in a shallow depression within the surface of the humerus, known as the radial groove.
During much of its course within the arm, it is accompanied by the deep branch of the brachial artery.
The axillary nerve lies near the posterior humerus and exists as one main trunk as it exits the quadrilateral space in the posterior upper arm. Complete paralysis of the deltoid may occur if the nerve is injured in this region.
Biomechanics of Shaft of Humerus Fracture
- Direct force
- Fall against a fixed object
- When a blunt object strikes the arm
- Produces a transverse type fracture line, occasionally with a nondisplaced butterfly fragment.
- Indirect force
- Energy absorbed by the humerus is through the distal portion of the limb.
- Twisting of the arm behind the back or during arm wrestling
- Create a spiral fracture.
- Muscular Forces
- Strong muscle contractions like throwing
- Spiral fractures
Major causes of fracture of shaft of humerus are
- Motor Vehicle accidents
- Fall from heights
- Direct trauma
Presentation of Shaft of Humerus Fracture

The patient presents with extreme pain at the site and skeletal instability. The patient often supports his injured limb with another one to ease the pain. On examination tenderness and swelling are noted.
The skin should be examined all around to not any wounds. If present, its communication should be noted with the fracture hematoma.
Neurovascular injuries are not very common with fracture humerus but must be looked for in every case. The vascular status of the extremity should be evaluated by palpation of distal pulses and assessment of capillary refill.
The radial nerve is quite vulnerable to injury in humeral fractures and must be evaluated along with an examination of other nerves. Motor testing of wrist dorsiflexion and of extension of the interphalangeal joint of the thumb along with sensory evaluation over the dorsum of the hand indicates whether the radial nerve is functioning normally.
Imaging
Anteroposterior and lateral views of the diaphysis, as well as views of the elbow and shoulder joints, should be done.
If there appears a compromise arterial Doppler examination should be done to rule out or confirm the injury.

Traction views may be necessary for fractures with significant shortening, proximal or distal extension but not routinely indicated

Treatment of Shaft of Humerus Fracture
Non-Operative Treatment
The majority of fractures of the shaft of humerus fractures can be managed non-operatively and has good union rate.
Criteria for acceptable alignment
- Less than 20° anterior angulation
- Less than 30° varus/valgus angulation
- Less than 3 cm shortening
Contraindications to nonoperative treatment are
- Severe soft tissue injury
- Arterial injury
- Associated limb injuries requiring surgery
Hanging Cast
With the elbow bent at 90 degrees, a long arm cast is placed and upper part of the cast is molded carefully to align the humeral fracture. A series of loops are incorporated into the cast at the junction of the middle and distal thirds of the forearm.
After application, the cast is then suspended by a strap around the neck connected to the loops on the cast.
By changing the position at which the strap connects to the loops, the alignment of the fracture can be adjusted.
The arm must remain dependent at all times. The patient should be sleeping in Fowler’s semi-reclining position, and while sitting, the patient should avoid support under the elbow.
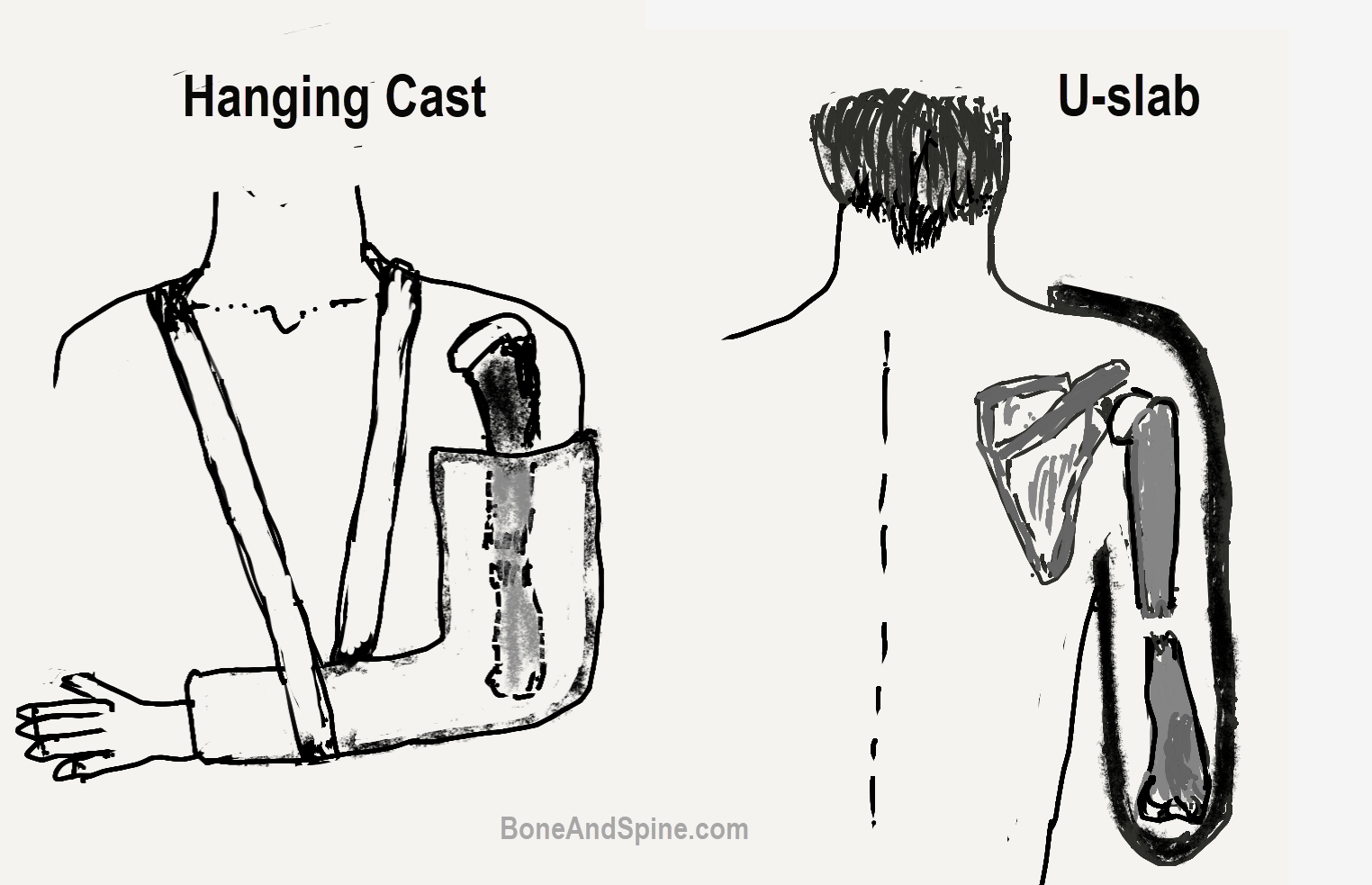
Coaptation splint followed by functional brace
It involves the placement of a well-molded plaster slab from the axilla or U-splint around the elbow, and over the deltoid with the elbow flexed to 90 degrees. A collar-and-cuff suspension sling supports the forearm. The splint is applied till the swelling resolves.
It is followed by the application of humeral fracture orthosis.
A rigid, light-weight plastic brace composed of an anterior and posterior shell joined by Velcro straps.
The splint extends from the axilla medially to a position as far distal as possible without limiting the motion of the elbow joint. {2.5 cm distal to axilla to 2.5 cm proximal to humeral condyles].
A flare extending over the deltoid with an additional strap meant to extend around the thorax may prevent the brace from slipping distally.
The sling should is not used. This allows gravity-assisted fracture reduction shoulder extension.
Weekly x-rays are done to check the reduction for 3-4 weeks and then at 2 weeks intervals.

As healing progresses, the patient is encouraged to do active range-of-motion exercises of the elbow joint as well as pendulum and circumduction exercises of the shoulder.
Bracing should be continued for at least 8 weeks to prevent refracture.
Surgical Treatment of Shaft of Humerus Fracture
Indications for Surgery
In the following situations, an operative intervention needs to be considered.
Absolute Indications [Surgery is absolutely necessary]
- Open fracture
- An arterial injury that needs repair
- Injury to brachial plexus
- Floating elbow ie. ipsilateral forearm fracture
Relative Indications [Surgery is considered on cases to case basis]
-
- Greater than 20° anterior angulation
- Greater than 30° varus/valgus angulation
- Greater than 3 cm shorteningInability to maintain acceptable fracture alignment with functional bracing.
- Associated conditions
- Multiple injuries
- Multiple long bones fractures
- Concomitant lower extremity fractures
- Injuries requiring prolonged recumbency
- Bilateral humerus fractures
- Pathological fracture
- Segmental fractures
- Fracture Configuration
- Distraction at fracture site [the bones do not rescue near enough]
- Intraarticular extension
- Soft tissue injury that does not allow bracing
The choice of treatment varies with the location and pattern of shaft of humerus humerus. Open reduction and internal fixation with plating/nailing is the standard treatment. Closed reduction and internal fixation with humerus nail can be done in suitable fractures.
Techniques of Surgical Fixation
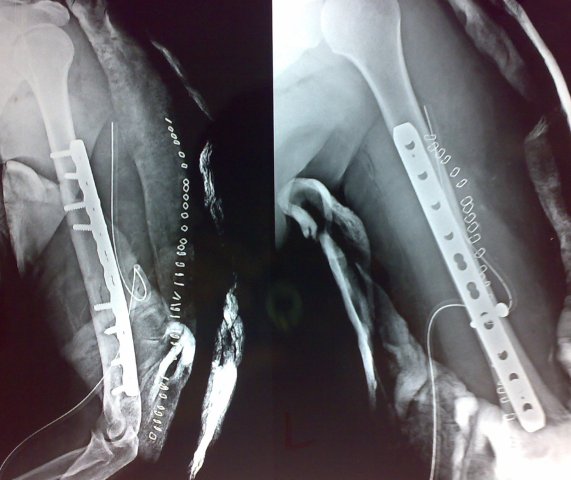
Compression Plating
This method involves fixing the fracture using a plate and screws. It is quite an effective method of fracture fixation but involves quite a significant amount of dissection and soft tissue stripping from the bone and at times may cause blood loss.
Anterolateral approach to humerus is used for proximal third to middle third shaft fractures.
The posterior approach to humerus is used for distal to middle third shaft fractures.
The choice of approach would also depend on the presence of elbow motion. If elbow motion is present, plate needs to be applied on anterolateral surface as that is the tensile surface.
When elbow is fixed and stiff the biomechanics become such that posterior aspect is tensile surface and plate should be applied on that surface.
Conventionally 4.5 mm screws in narrow direct compression plate are used. However, some studies have pointed 3.5 mm plates to be effective as well.
The most common complications reported with plating procedures are infection and iatrogenic radial nerve palsy. The range of motion of the elbow and shoulder of the involved extremity returns predictably after plate fixation.
Intramedullary Nailing
Intramedullary fixation with a nail involves passing a nail across the fracture sites. The intramedullary device could be multiple, flexible devices or a single, more rigid nail, usually with interlocking capability.
Nailing can be antegrade or retrograde. IM nailing associated with higher total complication rates of shoulder pain, nerve injury [radial nerve, musculocutaneous nerve].
External Fixation

Limited role in closed fractures. External fixation involves a system of pins and rods. The pins are passed inside the bone on either side of the fractures and held with connecting rods.
External fixation is used for open humerus fractures and in case of damage control orthopedics where definitive treatment is not possible.
Treatment of Open Fractures of Shaft of Humerus
An open fracture is one that has an associated wound over it and that wound communicates with fracture hematoma.
External fixation usually is done for fractures with such severe injury to the soft tissues and profound contamination.

Complications of Shaft of Humerus Fracture
Radial Nerve Palsy
The radial nerve gets injured in 6 to 15% of the fracture humeral shaft. Most of these palsies occur at the time of injury and would be identified at the time of first evaluation. Most palsies occur at the time of the injury and are identified at the initial evaluation of the fracture
10-20% of radial nerve palsies occur during the course of treatment.
Patients of shaft of humerus fracture would have a wrist drop in addition to humerus fracture. The patient would be unable to dorsiflex his wrist and extend the metacarpophalangeal joint.
The patient has a loss of grip strength and wrist and finger extension power. A wrist dorsiflexion splint dramatically improves grip strength and function and should be used on all patients. A functional splint with outrigger attachments to provide a passive extension of the digits through rubber bands is useful.
These should be given to every patient with radial nerve palsy.
Most of the patients just need to be observed while they recover uneventfully.
The patients where nerve does not show any recovery are benefited from tendon transfer surgery.
Nonunion
Fracture of shaft of humerus is very amenable to treatment but a percentage of fractures do not heal. Normal healing of a humeral fracture occurs over 8 to 10 weeks. If the fracture has not achieved union by 3 to 4 months, it can be considered a delayed union. If the union does not occur by 6 to 8 months it is called the nonunion of the fracture.
More on nonunion



There are various factors that increase the chance of whether a patient would develop non-union. These factors are
- Inadequate immobilization
- Distraction at the fracture site results in a gap between fractured surfaces
- Energy of the injury
- Open fractures


In the case of nonunion and osteoporosis, it might be difficult to meet the fixation. In such cases, an additional procedure like filling the capability with cement or augmentation with fibula may be needed.

Varus angulation is common but rarely has a functional deficit.
References
- Ekholm R, Adami J, Tidermark J, Hansson K, Törnkvist H, Ponzer S. Fractures of the shaft of the humerus. An epidemiological study of 401 fractures. J Bone Joint Surg Br. 2006 Nov. 88 (11):1469-73. Link
- Mahabier KC, Vogels LM, Punt BJ, Roukema GR, Patka P, Van Lieshout EM. Humeral shaft fractures: retrospective results of non-operative and operative treatment of 186 patients. Injury. 2013 Apr. 44 (4):427-30.
- Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop. 2010 Apr. 81 (2):216-23.
- Perez EA. Fractures of the shoulder, arm, forearm. Daugherty K, Jones L, eds. Campbell’s Operative Orthopaedics. 13th ed. Philadelphia: Elsevier; 2017. 2927-3016.
- Sims SH, Smith SE. Intramedullary nailing of humeral shaft fractures. J South Orthop Assoc. 1995 Spring. 4 (1):24-31.
- Mostafavi HR, Tornetta P 3rd. Open fractures of the humerus treated with external fixation. Clin Orthop Relat Res. 1997 Apr. (337):187-97.
- Verga M, Peri Di Caprio A, Bocchiotti MA, Battistella F, Bruschi S, Petrolati M. Delayed treatment of persistent radial nerve paralysis associated with fractures of the middle third of humerus: review and evaluation of the long-term results of 52 cases. J Hand Surg Eur Vol. 2007 Oct. 32 (5):529-33.
- Green E, Lubahn JD, Evans J. Risk factors, treatment, and outcomes associated with nonunion of the midshaft humerus fracture. J Surg Orthop Adv. 2005 Summer. 14 (2):64-72.