Last Updated on November 22, 2023
The shoulder is actually composed of four joints, namely glenohumeral joint, acromioclavicular joint, sternoclavicular joint and scapulothoracic joint. In common usage, shoulder joint mostly refers to the glenohumeral joint, the major joint of the shoulder but can also include acromioclavicular joint.
The shoulder joint is the most mobile joint in the human body and responsible for movements of arm and scapula.
The joint is very mobile and for attaining so much mobility, the stability of the shoulder joint has been compromised by the body. This instability is compensated for by rotator cuff muscles, tendons, ligaments, and the glenoid labrum.
Bones of Shoulder Joint
The shoulder is composed of the bones scapula clavicle and humerus.
Scapula
The scapula is a thin triangular bone that functions mainly as a site for muscle attachment and origin. It takes part in the formation of the glenohumeral, acromioclavicular and scapulothoracic joint. It also provides orignin t0 roator cuff muscles.
[Detailed anatomy of scapula ]
Clavicle
The clavicle is an S-shaped bone and has two articulations, the sternoclavicular joint, and the acromioclavicular joint and serves to connect trunk with the upper limb.
[Detailed anatomy of clavicle]
Humeral head
Head of the humerus forms the proximal articular surface of the humerus that articulates against the shallow glenoid cavity. Only one-fourth of head makes contact with glenoid cavity. Glenoid labrum is a fibrocartilaginous ring attached to the outer rim of the glenoid cavity, provides additional depth and stability.
Following video gives an idea of the arrangement of the bones
Joints of Shoulder
There are three joints of the shoulder- glenohumeral, acromioclavicular, and the sternoclavicular joints.
Sternoclavicular joint
This joint is formed by the medial end of the clavicle with the manubrium or topmost portion of the sternum [see the video above]. The costoclavicular ligament is the main stabilizer of the joint. A fibrocartilaginous disc present at the joint increases the range of movement.
The sternoclavicular joint is the sole connection between the axial skeleton and the upper extremity. The sternoclavicular joint allows 30-35 degrees of upward elevation, 35 degrees of anteroposterior movement, and 44-50 degrees of rotation about the long axis of the clavicle.
Acromioclavicular Joint
The acromioclavicular joint is the sole joint acromion clavicle and scapula [via acromion process]. The joint, a diarthrodial joint itself has a little movement. It is held together by its joint capsule and the coracoacromial ligaments: the trapezoid and conoid ligaments.
Glenohumeral Joint
The glenohumeral joint is ball-and-socket synovial joint formed by the articular surfaces of the glenoid cavity and the head of the humerus. It is the main joint of the shoulder and allows the arm to rotate in a circular fashion or to hinge out and up away from the body. The shoulder joint is very mobile because glenoid fossa is shallow but this also adds to the instability of the shoulder.
The glenoid cavity depth is increased by a rim of fibrocartilage called glenoid labrum which is composed of dense fibrous tissue. The average depth of the glenoid cavity is 2.5 mm, but the labrum serves to increase this depth.
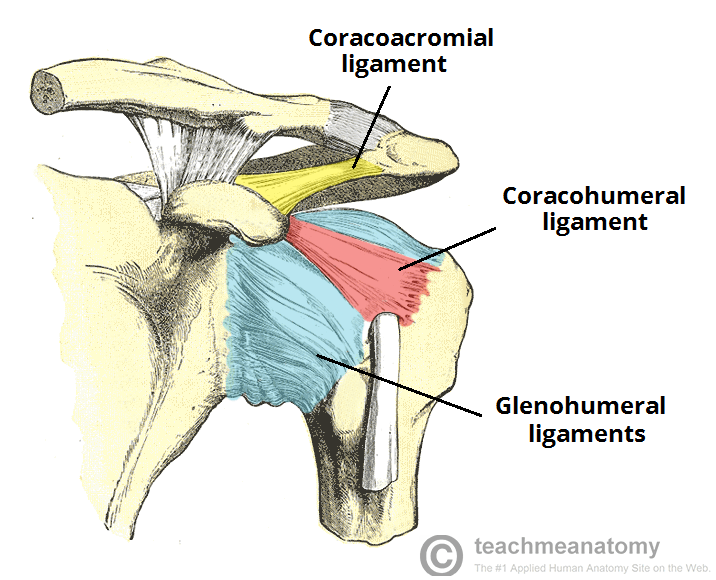
The capsule of the glenohumeral joint the joint and attaches to the scapula, humerus, and head of the biceps. It is lined by a thin, smooth synovial membrane. Coracohumeral ligament attaches the coracoid process of the scapula to the greater tubercle of the humerus. Glenohumeral ligaments are three ligaments that attach the lesser tubercle of the humerus to the lateral scapula.
Semicirculare humeri is a transversal band between the posterior sides of the lesser tuberosities of the humerus.
Scapulothoracic Joint
The scapulothoracic joint is not a true joint. Scapulothoracic articulation is formed by the convex surface of the posterior thoracic cage and the concave surface of the anterior scapula and its movements are determined by the integrity of sternoclavicular and acromioclavicular joints.
Ligaments of Shoulder Joint
Coracoclavicular Ligaments
There are two coracoclavicular ligaments – conoid and trapezoid which maintain the articulation of the clavicle with the coracoid process of the scapula. Coracoclavicular ligaments are the primary restraint to superior and posterior acromioclavicular dislocation.
Glenohumeral Ligaments
There are three glenohumeral ligaments
- Superior glenohumeral ligament
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
The superior glenohumeral ligament has a variable origin on the lateral aspect of scapula and inserts on the humerus near the lesser tubercle. Superior glenohumeral ligament resists downward translation of the humeral head in the adducted shoulder.
Middle glenohumeral ligament originates from the labrum and inserts on the humerus medial to the lesser tubercle. This ligament resists inferior translation when the humeral head is in the adducted and externally rotated shoulder.
Inferior glenohumeral ligament originates from the labrum and the adjacent glenoid neck inserts on the anatomic neck of the humerus. It resists anterior and posterior translation of humeral head. This ligament resists inferior translation in the abducted shoulder.
Coracohumeral Ligament
The coracohumeral ligament originates on the base and lateral border of the coracoid process of the scapula and inserts on the greater tubercle. It appears to have a suspensory function of the humeral head.
Major Muscles of the Shoulder
Serratus Anterior
Serratus anterior originates on the surface of the upper eight ribs at the side of the chest and inserts along the anterior length of the medial border of the scapula. It fixes the scapula into the thoracic wall and aids in rotation and abduction of the shoulders.
Subclavius
This muscle originates from first rib and inserts in the subclavian groove of the clavicle. It acts as a stabilizer of the clavicle and also depresses the lateral clavicle.
Pectoralis Minor
Pectoralis minor arises from the third, fourth, and fifth ribs, near their cartilage and inserts into the medial border and upper surface of the coracoid process of the scapula.
It helps in respiration, cause medial rotation of the scapula, causes protraction of the scapula, and draws the scapula inferiorly.
Sternocleidomastoid
Sternocleidomastoid attaches to the sternum and clavicle on one side and the mastoid process [bony projection of the temporal bone of the skull.]
It acts to flex and rotate the head. It also aids in respiration by elevating the sternoclavicular joint when the head is fixed.
Levator Scapulae
Levator scapulae arise from the transverse processes of the first four cervical vertebrae and inserts into the medial border of the scapula.
Levator scapulae elevates and rotates the scapula.
Rhomboids
Rhomboid major and rhomboid minor muscles work together. They arise from the spinous processes of T1 to T5 vertebrae and spinous processes of the seventh cervical vertebra. Rhomboid major and rhomboid minor insert on the medial border of the scapula. They cause adduction and downward rotation of the scapula.
Trapezius
Trapezius is a large muscle that arises from the occipital bone, the ligamentum nuchae, the spinous process of the seventh cervical, and the spinous processes of all the thoracic vertebrae, and from the corresponding portion of the supraspinal ligament. It inserts on the lateral clavicle, the acromion process, and into the spine of the scapula.
Trapezius is involved in depression, upward rotation, elevation, and adduction of scapula acting through different parts.
Deltoid
Anterior deltoid fibers arise from the anterior border and the upper surface of the lateral third of the clavicle. Middle fibers arise from the lateral margin and upper surface of the acromion. Posterior fibers arise from the lower lip of the posterior border of the spine of the scapula.
Deltoid is powerful shoulder abductor. Anterior fibers are involved in shoulder abduction when the shoulder is externally rotated. Anterior deltoid also assists the pectoralis major during shoulder transverse flexion movement.
The middle fibers abduct the shoulder when the shoulder is internally rotated and are involved in shoulder transverse abduction.
The posterior fibers are strongly involved in transverse extension and also hyperextend the shoulder.
Rotator Cuff
Supraspinatus, subscapularis, infraspinatus, and teres minor form the rotator cuff and contribute to the stability of the shoulder. The four tendons of these muscles converge to form the rotator cuff tendon. These tendinous insertions along with the articular capsule, the coracohumeral ligament, and the glenohumeral ligament complex, blend into a confluent sheet before insertion into the humeral tuberosities.]
Rotator cuff stabilizes the glenohumeral joint and causes external rotation of the humerus.
Capsule and Bursae of Shoulder Joint
The joint capsule is a lax fibrous sheath extends from the anatomical neck of the humerus to the border of the glenoid fossa. The joint capsule is lined by the synovial membrane and produces synovial fluid to reduce friction between the articular surfaces.
Bursa is a synovial fluid-filled sac that acts as a cushion between tendons and other joint structures. Subacromial bursa is located inferior to the deltoid and acromion, and superior to the supraspinatus tendon and the joint capsule.

Subscapular bursa is located between the subscapularis tendon and the scapula. It reduces wear and tear on the tendon during movement at the shoulder joint.
Movements of Shoulder
Sternoclavicular joint, acromioclavicular joint, glenohumeral joint, and scapulothoracic joint work together to carry out movements shoulder motion. The majority of motion occurs at the glenohumeral and scapulothoracic joints and a rhythm between these two is present.
The ratio of glenohumeral to scapulothoracic of total shoulder motion is 2:1. [This value is average value and is not constant in entire arc of motion.] In the initial portion of abduction, glenohumeral motion occurs more [4:1} and after the shoulder moves above 90° of abduction, it decreases to 1:1.
During the motion, the shoulder is stabilized by
- Static stabilizers [bony structures, labrum, GH ligaments, and joint capsule]
- Dynamic stabilizers [rotator cuff [the supraspinatus, infraspinatus, subscapularis, and teres minor], and scapular stabilizers (ie, teres major, rhomboids, serratus anterior, trapezius, levator scapula).
The following describes the terms used for different movements of the shoulder – [ See the video that follows for a demonstration of the movement.]
Arm Flexion
The humerus is rotated out of the plane of the torso so that it points forward. Pectoralis major, coracobrachialis, biceps brachii, anterior fibers of deltoid are main muscles that are involved.
Arm Extension
The humerus is rotated out of the plane of the torso so that it points backwards. Latissimus dorsi and teres major, long head of triceps, posterior fibers of the deltoid are main muscles that are involved.
Arm Abduction
Arm abduction occurs when the arms are held at the sides, parallel to the length of the torso, and are then raised in the plane of the torso. This movement may be broken down into two parts: True abduction of the arm, which takes the humerus from parallel to the spine to perpendicular; and upward rotation of the scapula, which raises the humerus above the shoulders until it points straight upwards. Supraspinatus (first 15 degrees) and deltoid act to abduct whereas upward rotation of scapula is by trapezius and serratus anterior.
Arm Adduction
Arm adduction is the opposite motion of arm abduction. It can be broken down into two parts: downward rotation of the scapula and true adduction of the arm.
Downward rotation of scapula is caused by pectoralis minor, pectoralis major, subclavius and latissimus dorsi whereas true adduction is caused by teres major and the lowest fibers of the deltoid.
Medial rotation of the arm
Medial rotation turns the arm inwards. when the elbow is held at a 90-degree angle and the fingers are extended so they are parallel to the ground. Medial rotation occurs when the arm is rotated at the shoulder so that the fingers change from pointing straight forward to pointing across the body. Subscapularis, latissimus dorsi, teres major, pectoralis major, anterior fibers of deltoid are the main muscles.
Lateral rotation of the arm
The opposite of medial rotation of the arm. Muscles used are infraspinatus and teres minor, posterior fibers of deltoid.
Arm Circumduction
Movement of the shoulder in a circular motion so that if the elbow and fingers are fully extended the subject draws a circle in the air lateral to the body. Pectoralis major, subscapularis, coracobrachialis, biceps brachii, supraspinatus, deltoid, latissimus dorsi, teres major and minor, infraspinatus, long head of triceps are the muscles used in circumduction.
Horizontal Extension or Abduction
This movement is opposite of the previous movement Lateral movement away from the midline of the body in a horizontal plane; moving the upper arm away from the chest. Deltoid, infraspinatus and teres minor participate in this movement.
Horizontal Flexion or Adduction
Horizontal adduction is the medial movement toward the midline of the body in a horizontal plane. It moves the upper arm toward and across the chest. The muscles involved are pectoralis major and coracobrachialis.
Scapular Elevation
The scapula is raised in a shrugging motion by use of levator scapulae, the upper fibers of the trapezius.
Scapular Depression
The scapula is lowered from elevation. The scapulae may be depressed so that the angle formed by the neck and shoulders is obtuse, giving the appearance of “slumped” shoulders. Muscles used are pectoralis minor, lower fibers of the trapezius, subclavius, latissimus dorsi.
Scapular Protraction or Scapular Abduction
The opposite motion of scapular retraction. The scapula is moved anteriorly and laterally along the back, moving the arm and shoulder joint anteriorly. If both scapulae are protracted, the scapulae are separated and the pectoralis major muscles are squeezed together. Muscles used are serratus anterior (prime mover), pectoralis minor and major.
Scapular Retraction or Scapular Adduction
The scapula is moved posteriorly and medially along the back, moving the arm and shoulder joint posteriorly. Retracting both scapulae gives a sensation of “squeezing the shoulder blades together. Muscles used are rhomboideus major, minor, and trapezius.