Last Updated on March 14, 2021
Sternoclavicular joint injury is quite rare and results from the direct or indirect force on the sternoclavicular joint. . The sternoclavicular joint is a plane synovial joint formed by the articulation of the sternum and the clavicle. Interestingly, it is the only bony joint that connects the axial with the appendicular skeleton.
Sternoclavicular injuries are rare. Most injuries consist of anterior dislocations which are about 20 times more common than posterior. But the posterior dislocations are of a more serious nature as the clavicle moves toward the thorax and may cause severe symptoms.
Anterior sternoclavicular joint dislocations often result in pain, functional limitations, or cosmetic issues.

Posterior sternoclavicular joint dislocations can be life-threatening due to complications like airway, neurovascular injury, and esophageal injury.
Sternoclavicular injuries are more common is increased in young adult males.
Relevant Anatomy
To locate the sternoclavicular joint, just palpate the clavicle or collarbone medialward. The medial end of the clavicle is the approximate region of this joint where it articulates with the clavicular notch of the sternum. The sternum has two clavicular notches on either side of the superior end for clavicles.
The clavicles are well received in these notches and held by ligaments. There is an intraarticular disc between two articulating surfaces.
Sternoclavicular joint dislocation results in prominence of medial clavicle end.

The sternoclavicular joint has little inherent stability but is supported by strong joint capsule ligaments. The capsule surrounding the joint is weakest inferiorly.
The ligaments of the joint include
- Interclavicular ligament
- Anterior and posterior sternoclavicular ligaments
- Costoclavicular ligaments
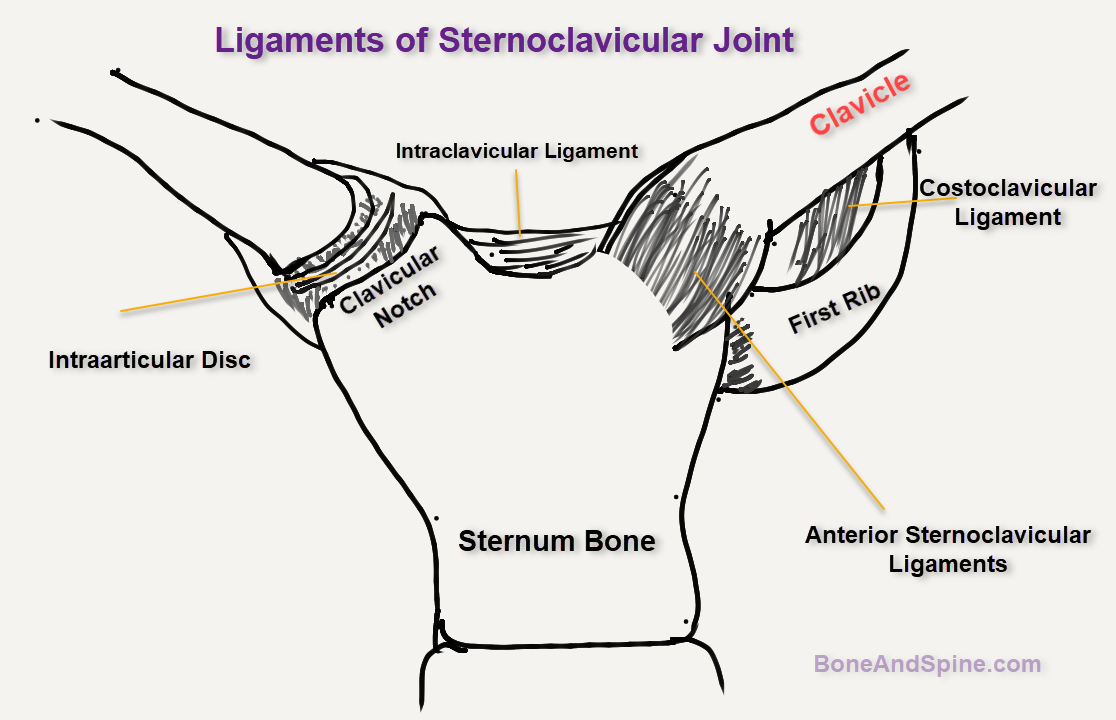
The anterior and posterior sternoclavicular ligaments originate from the anterior and posterior aspects of the medial end of the clavicle, respectively.
These respectively insert onto the anterior and posterior surfaces of the manubrium.
The interclavicular ligament connects the superomedial portions of each clavicle.
The articular branches of the internal thoracic and suprascapular arteries are responsible for the blood supply of the sternoclavicular joint.
The costoclavicular ligament provides joint stability.
It is a short, flat ligament that in form that attaches below to the upper and medial part of the cartilage of the first rib.
It goes posterolaterally to attach to the costal tuberosity on the inferior aspect of the clavicle.
Nerve supply is by the branches of the medial suprascapular nerve.
Important posterior vascular relations of the sternoclavicular joint are
- Brachiocephalic trunk
- Common carotid artery
- Internal jugular vein
Hence, posterior dislocation of the joint may put these structures at risk of injury.
The sternoclavicular joint provides mobility in two planes mainly an upward-downward movement of clavicle and front-back displacement of the clavicle. There is mild rotational movement too, making it have three degrees of freedom.
Pathophysiology
Mechanisms of Sternoclavicular Joint Injury
It requires a substantial force to dislocate a sternoclavicular joint.
It can happen by way of direct force or indirect force
- Direct Force
- Force on the anteromedial aspect of the clavicle
- The clavicle is pushed posteriorly behind the sternum
- Results in posterior dislocation
- Indirect Force
- Indirect force on the sternoclavicular joint
- From the anterolateral or posterolateral aspects of the shoulder
- Most common mechanism
- Can result in both types of dislocations
- Shoulder compressed and rolled forward- posterior dislocation
- Shoulder compressed and rolled backward – Anterior dislocation
Causes
- Motor vehicle accidents [Most common cause]
- Fall on an outstretched abducted arm- drives the shoulder medially
- Congenital, degenerative, and inflammatory processes
- High contact sports
Patients with ligamentous laxity may be prone to this injury.
Associated Injuries
- Anterior dislocation
- Pneumothorax
- Hemothorax
- Rib fractures
- Lung contusion
- Posterior dislocation
- Vascular injury like subclavian artery
- Pneumothorax
- Esophageal injury
- Cardiac arrhythmias
- Brachial plexus injury
- Airway injury
Classification of Sternoclavicular Joint Injury
- Mild Sternoclavicular Joint Injury- Sprain
- Intact ligaments
- Mild to moderate amount of pain especially with limb movements
- Mild swelling and pain
- No instability
- Moderate Sternoclavicular Joint Injury- Subluxation
- Partially disrupted or severely stretched ligaments
- Marked swelling and pain esp on limb movement
- Comparison with the opposite site may suggest displacement of joint
- Severe Sternoclavicular Joint Injury- Dislocation
- Frank dislocation
- The capsular ligament and the intraarticular disk ligament are ruptured.
- All features of subluxations are present with increase severity
There is another type of sternoclavicular joint injury called atraumatic subluxation and dislocations.
These are usually anterior and are usually painless. The patient raises the arm forward, the medial clavicle spontaneously displaces anteriorly and superiorly, and there is a reduction of the medial clavicle when arm is lowered.
Clinical Presentation of Sternoclavicular Joint Injury
In an acute injury, the patient complains of pain in the chest and shoulder region. The head is tilted towards the affected side. The pain worsens on the movement of the arm and when the person is in the supine position.
Pain tends to be more severe with posterior dislocations.
Other associated symptoms that may be present are
- Difficulty in breathing
- Difficulty in swallowing
[In unconscious patients, the injury should be suspected in cases of swelling in the region and should be investigated accordingly so as not to miss the severe injury.]
Shock and pneumothorax may be present in posterior dislocations of the sternoclavicular joint.
The affected shoulder usually appears shortened and thrust forward. Chest of the patient should be examined in detail especially when there is tachypnea, stridor, hoarseness and other signs of respiratory distress.
The limb should be examined for neurovascular status.
It must be noted that posterior dislocations are more subtle in appearance at the injury site but the risk of other injuries is substantial.
Imaging in Sternoclavicular Joint Injury
Xrays
Anteroposterior x-rays of the chest or sternoclavicular joint may show sternoclavicular joint displaced as compared with the normal side. Lateral x-rays are difficult to interpret due to overlapping of structures.
Special X-rays for better visualization are discussed as follows.
Heinig View, Hobbs View, and Serendipity View are special views done to confirm this injury
If the sternoclavicular joint is dislocated anteriorly, the affected clavicle will appear to be displaced and riding higher. If it is dislocated posteriorly, it will appear to be lower.
CT Scan
CT scan is the best modality to study sternoclavicular joint injury. It helps to distinguish articular injuries of the joint from fractures of the medial clavicle.
Other Studies
Angiography or esophagoscopy may be needed in posterior dislocations.
Treatment of Sternoclavicular Joint Injury
Nonoperative treatment includes analgesic medication and other supportive treatments.
Anterior Sternoclavicular Joint Injury
Mild anterior sternoclavicular injuries are often stable. Ice application for 12 -24 hours followed by immobilization of the limb is done for 4 days to one week. Following that the limb should be gradually used in day-to-day activities.
Moderate injuries [subluxation] can be reduced by drawing the shoulders backward. Once the reduction occurs the limb is immobilized for about 2 weeks.
A clavicular immobilizer is used to hold the reduction. Alternatively, a figure of 8 bandage can be used.
Severe injury means dislocation. A treatment approach similar to subluxations can be tried but often is not successful and the patient often requires surgery.
For closed reduction, under local or general anesthesia or sedation, the patient is placed supine on the table. Keep a thick pad between the shoulders. Reduce the joint with direct gentle pressure over the anteriorly displaced clavicle while an assistant pushes both the shoulders back to the table.
After reduction, the shoulders should be held back for 4 to 6 weeks with a figure-of-eight dressing. Gradual mobilization is begun after that.
Posterior Sternoclavicular Joint Injury
Posterior sternoclavicular joint injury is more dangerous than anterior sternoclavicular injuries.
For mild to moderate injuries, a figure-of-eight bandage for 2 to 6 weeks is applied for immobilization.
Severe injury or dislocation may be accompanied by damage to the structures posterior to the joint and a detailed evaluation should be done.
A nonoperative approach may be tried especially in young adults.
Under general anesthesia or sedation, the closed reduction should preferably be done within 48 hours.
The abduction traction technique is the most commonly used technique for reduction.
The patient is placed on his back with the dislocated shoulder near the edge of the table. A thick sandbag is placed between the shoulders.
Lateral traction is applied to the abducted arm, which is then gradually brought back into extension. The clavicle usually reduces with an audible snap or pop, and it is almost always stable.
Operative treatment of posterior sternoclavicular dislocation should be considered when the dislocation is not reducible.
The surgery involves the reduction and augmentation of joint ligaments by the use of tissue such as fascia lata or subclavius tendon.
The suture can also be used.
Other described procedures are osteotomy, arthrodesis, and resection of the medial end of the clavicle.
References
- Dhawan R, Singh RA, Tins B, Hay SM. Sternoclavicular joint. Shoulder Elbow. 2018 Oct. 10 (4):296-305.
- Hellwinkel JE, McCarty EC, Khodaee M. Sports-related sternoclavicular joint injuries. Phys Sportsmed. 2019 Sep. 47 (3):253-261.
- Sernandez H, Riehl J. Sternoclavicular Joint Dislocation: A Systematic Review and Meta-analysis. J Orthop Trauma. 2019 Jul. 33 (7):e251-e255.
- Yeh GL, Williams GR. Conservative management of sternoclavicular injuries. Orthop Clin North Am. 2000 Apr. 31(2):189-203.
- Tepolt F, Carry PM, Heyn PC, Miller NH. Posterior sternoclavicular joint injuries in the adolescent population: a meta-analysis. Am J Sports Med. 2014 Oct. 42 (10):2517-24.
- Van Hofwegen C, Wolf B. Suture repair of posterior sternoclavicular physeal fractures: a report of two cases. Iowa Orthop J. 2008. 28:49-52.