Last Updated on October 29, 2019
Thumb injuries or fractures and dislocations are one of the common hand injuries. The term thumb injury includes all the injuries from the carpometacarpal joint to the tip of the thumb.
There are various types of thumb injuries that come under fractures and dislocations of thumb. Nailbed and fingertip injuries are discussed separately.
Thumb is an important organ and makes the human hand a highly efficient tool. An unusable thumb could mean a loss of 40% of hand function.
Thumb injuries mostly occur in children and the elderly. In fact, in the elderly, the thumb is the most common tubular bone fractured in the hand.
Thumb injury results from both direct and indirect trauma with the motor vehicle and bicycle accidents are the most common causes.
Relevant Anatomy
The thumb makes our hand a very efficient organ. This is achieved by its unique structure and plane of movements.
THumb consists of two phalanges and a metacarpal, which articulates with the trapezium bone.
The MCP joint has 6 degrees of freedom. It produces motion of
- Flexion and extension
- Abduction and adduction
- Pronation and supination
The carpometacarpal joint is an articulation between the trapezium and the metacarpal base. Following ligaments provide the stability-
- Volar and dorsal oblique ligaments
- Volar oblique originates on the trapezium and inserts into the volar beak of the thumb metacarpal.
- The most important ligament in maintaining stability
- The dorsal ligament is not as strong as volar
- The dorsal ligament is reinforced by abductor pollicis longus
- Anterior and posterior intermetacarpal ligaments
- Dorsal radial ligament
Metacarpal bone consists of a base, shaft, and head. The head contains an articular surface for the base of the proximal phalanx to form the metacarpophalangeal joint.
This joint is supported laterally by-
- The proper collateral ligament
- Arises from the lateral condyles of the metacarpal
- Inserts on the volar aspect of the proximal phalanx
- Tight in flexion and loose in extension
- Accessory collateral ligament
- Arises from the metacarpal neck
- Inserts into the volar plate and the sesamoids
- More volar in location than the proper collateral ligament
- Tight in extension and loose in flexion
The interphalangeal joint of the thumb functions as a hinge and has motion in flexion and extension. The stability of the interphalangeal joint is provided by the collateral and accessory collateral ligaments as well as the trochlear shape of the joint. A thick fibrocartilaginous structure provides volar support and is called a volar plate.
A single sesamoid could be present within the volar plate at the interphalangeal joint.
Types of Thumb Injuries
Thumb injuries can be of following types
- Injuries to phalanges
- Phalangeal fractures
- Mallet thumb
- Interphalangeal joint dislocations
- Metacarpal injuries
- Metacarpophalangeal dislocations
- Metacarpal fractures
- Thumb carpometacarpal dislocations
- Thumb metacarpophalangeal joint ulnar collateral ligament injuries (Skier’s thumb)
Pathophysiology of Different Thumb Injuries
Phalangeal fractures of Thumb

The thumb is formed of two phalanges- the distal and proximal phalanx. Fractures of these phalanges are generally diagnosed and treated identically to phalangeal fractures of the other digits.
Mainly speaking phalangeal fractures of thumb is
- Distal phalanx fractures
- Extra-articular tuft fractures
- Often caused by a crush injury
- Intra-articular tendon avulsion injuries. Tuft fractures generally are caused by a crush injury to the distal thumb.
- Secondary to avulsion of the extensor tendon
- Proximal phalanx fractures
- Fractures of the phalangeal head and shaft.

Mallet thumb
Closed mallet thumb injuries are not common. It usually occurs secondary to an acute forceful flexion of the thumb interphalangeal joint causing avulsion of the extensor tendon.
Like mallet finger, mallet thumb may occur with or without distal phalangeal insertion.
In thumb, open mallet injury is more common due to the laceration of the tendon.
Thumb Interphalangeal Joint Dislocations
- Rare and usually dorsal
- Hyperextension and rotational injury
- The interposition of the palmar plate, secondary to rupture of this structure may cause failure to reduce
Thumb Metacarpophalangeal Dislocations
Dorsal dislocations are much more common and occur due to hyperextension injury occurring either by falling on an outstretched hand or axial loading to the tip of the thumb. Dorsal dislocation causes tearing of the volar plate which may interpose leading to an irreducible dislocation.
Volar dislocations are less common but often irreducible due to the interposition of the dorsal capsule and tendon of either the extensor pollicis longus or the extensor pollicis brevis.
Thumb metacarpal fractures
Thumb metacarpal fractures can be of the head, shaft or base.
- Fractures of the head are rare and often occur due to direct trauma.
- Shaft fractures often follow high energy injury but are uncommon. These fractures often result in shortening and malrotation.
- Base fractures of thumb metacarpal are common. These are caused by an axial loading on a slightly flexed metacarpal shaft.
The base fractures are further divided into
- Extra-articular
- Occur at the proximal metaphyseal-diaphyseal junction
- Distal fragment adducted and flexed due to pulling of
- Adductor pollicis
- Abductor pollicis Brevis,
- Flexor pollicis Brevis.
- Divided into transverse and oblique fractures
- Intra-articular fractures
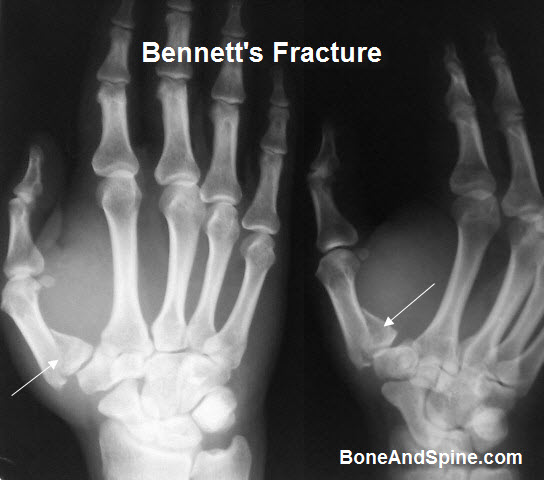
- Bennett fracture
- Intra-articular basilar fracture of the thumb metacarpal
- A single volar ulnar base portion remains intact.
- Intact fragments held by the volar oblique ligament
- The displaced metacarpal is pulled dorsally and radially by the abductor pollicis longus, adductor pollicis, and thumb extensors
- Rolando fracture
- 3-part intra-articular base fracture of the base of the thumb.
- T or Y pattern fracture with both volar and dorsal fragments is present
- The least common type of the metacarpal base fractures
- Volar carpal ligament remains attached to the volar fragment
- Adductor pollicis longus remains with the dorsal fragment.
- Comminuted fractures.
- Quite common
- Produce varying degrees of
- articular surface impaction
- Bennett fracture
Thumb Carpometacarpal Dislocations
- Rare
- Can be accompanied by avulsion fracture [volar oblique ligament]
- Ligamentous disruption may occur and lead to prolonged hypermobility
Thumb MCP ulnar collateral ligament injuries
- Commonly called Skier’s thumb
- Occur due to extreme valgus stress to the thumb
- Rupture of ulnar collateral ligament
- Usually, the rupture is at the distal insertion
Presentation of Thumb Injuries
Pain, swelling, and deformity are common modes of presentations across all the injuries. The site of pain and deformity gives an idea of the injury.
Some injuries have their peculiar presentations.
- Mallet thumb presents with slightly flexed posture and an inability to extend the thumb at the interphalangeal joint.
- Dislocations are evident by their deformities and inability to move the involved joint. Dimpling, puckering, or abnormal skin crease suggests an irreducible dislocation.
- Skier’s thumb has a peculiar history of a valgus injury to the thumb. It is a common injury in skiers.
Imaging
X-rays of the thumb are taken with a focus on the digit are taken. In most cases AP and lateral views are sufficient. But special views may be needed.
- True AP of thumb (Robert’s View)
- Arm in full pronation with the dorsum of thumb on cassette
- True lateral of thumb
- hand pronated 30 degrees and beam angled 15 degrees distally
- Traction view
- For a better understanding of fracture pattern
- Especially done in Rolando and severely comminuted
Different findings are
- Fractures and dislocations will be evident
- Mallet thumb may show an avulsed fragment
- Bennet’s fracture is characterized by a small fragment of 1st metacarpal base articulating with trapezium
- Rolando fracture shows a typically Y shaped intraarticular fracture due to splitting of the metacarpal base into volar and dorsal fragments

Treatment of Thumb Injuries
Most of the closed injuries are amenable to reduction and splinting. Open injuries always require surgery. Specific treatments are discussed below.
Phalangeal fractures
- 20-30 degrees angulation in a lateral plane is acceptable
- Stable fractures are treated by splinting or buddy wrapping
- Nail injuries and fingertips injuries are often treated with surgical repair
- Unstable fractures require reduction and percutaneous fixations
- Irreducible closed fractures require open reduction
[Learn more about phalangeal fractures]
Mallet Thumb
- Usually does not require surgery
- Splint in extension for 6 weeks suffices
- Surgery is done for open injuries or in case of bony avulsion
- open injury, failed closed treatment, chronic injury and/or mal-union, or a mallet thumb with bony avulsion
[Read more about Mallet injury]
Interphalangeal and Metacarpophalangeal dislocations
Closed reduction is attempted in all dislocations.
If successful, the thumb is splinted to block the movement of the affected joint. That means in case of metacarpophalangeal dislocation the splint should extend to the wrist too.
Irreducible dislocations should be reduced by open surgery and jointly fixed in anatomical position with K-wires.
Metacarpal Fractures
- Metacarpal head fractures
- intra-articular
- ORIF if evidence of joint incongruity or displacement exists. Stable anatomic reduction allows for early motion and a reduced risk of post-traumatic stiffness and/or osteoarthritis.
- Metacarpal shaft fractures
- Stable fractures treated by closed reduction and IP splinting
- Open reduction
- shortening of more than 2 mm
- Angulation of greater than 20 degrees
- Rotation
- Open fractures.
- Metacarpal base fractures
- Extra-articular fractures
- Closed reduction and thumb spica cast
- Transverse fractures generally are stable
- Oblique fractures may displace
- Surgery indicated in
- Angulation greater than 30 degrees
- Comminuted fractures with shortening
- Open fractures.
- Bennett fracture
- `Closed reduction and thumb spica cast immobilization if the reduction is stable
- Otherwise closed or open reduction with k-wire fixation
- Greater than 1 mm of articular incongruity after closed reduction indicates operative intervention
- Rolando fracture
- The articular incongruity and fragment size determines the treatment pattern
- Nondisplaced fracture with articular incongruity less than 1 mm – percutaneous pin fixation
- More than 1 mm of incongruity
- Open reduction or distraction techniques
- Comminuted fractures
-
-
- Ligamentotaxis or distraction
-
-
- Skier’s thumb
- Acute incomplete ruptures
- Short arm thumb spica cast for 4 weeks.
- Surgical repair incompletein complete ruptures or old symptomatic ruptures
- Extra-articular fractures
Complications
- Stiffness
- Degenerative arthritis in nonanatomical reduction of intra-articular fractures
- Loss of motion
- Prolonged immobilization
- Adhesions
Prognosis
The severity of the initial injury determines the prognosis.
Anatomical restoration is associated with better function and decreased risk of complications.
References
- Stanton JS, Dias JJ, Burke FD. Fractures of the tubular bones of the hand. J Hand Surg Eur Vol. 2007 Dec. 32(6):626-36.
- Melone CP Jr, Beldner S, Basuk RS. Thumb collateral ligament injuries. An anatomic basis for treatment. Hand Clin. 2000 Aug. 16(3):345-57.
- Abid H, Shimi M, El Ibrahimi A, El Mrini A. Articular fracture of the base of the thumb metacarpal: comparative study between direct open fixation and extrafocal pinning. Chir Main. 2015 Jun. 34 (3):122-5.
- Soyer AD. Fractures of the base of the first metacarpal: current treatment options. J Am Acad Orthop Surg. 1999 Nov-Dec. 7(6):403-12.