Last Updated on October 28, 2023
Digital nerve blocks are used for numbing digits [fingers, toes] for a procedure on the digits. Injury and infection are the two most common reasons for surgical procedures of digits. The digital block is generally effective for procedures distal to metatarsal or metacarpal heads.
Relevant anatomy
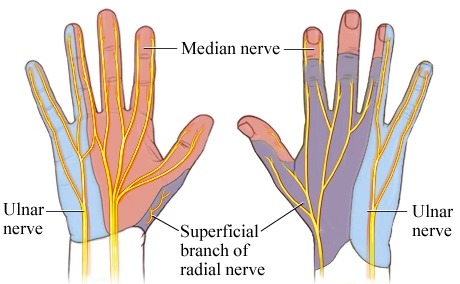
Each digit is innervated by 4 digital nerves – two dorsal and two palmar.
Median, ulnar, and radial nerves are responsible for the cutaneous supply of hand and digits. The two palmar digital nerves innervate the palmar aspect of the digit and the nail bed, whereas the dorsal nerves innervate the dorsum of the digit.
Digital nerves of the foot also follow a similar fashion. The tibial and peroneal nerves branch off into the digital nerves of the foot]
Indications of Digital Block
Any procedure of the digit not amenable to local infiltration is an indication of digital block. Some surgeons prefer digital block to local infiltration.
The procedure list is exhaustive but generally includes
- Large lacerations
- Nail bed injuries
- Ingrown nails
- Paronychia
- Fractures and dislocation of phalangeal fractures
Contraindications
The digital block should not be given if there is a compromised digital circulation, infection at the site of injection or there is a known allergy to anesthetic
Equipment
The equipment necessary includes the following:
- Sterile gloves and drapes
- Gauze pads, bandages
- Betadine solution
- Syringe, 5-10 mL
- 18-gauge needle for drawing up the anesthetic
- 25 to 30-gauge needle for injection
- Local anesthetic of choice
- Lidocaine
- Procaine
- Bupivacaine – long acting
Techniques of Digital Block
Various methods of giving digital block are
- Web-space block
- Transthecal block
- Three-sided digital block
- Four-sided ring block.
Following things should be kept in mind
- Follow standard sterile precautions in all the procedures
- Do not use epinephrine or adrenaline
- Use the smaller needle for injections. This leads to less pain.
- Use appropriate amount for the space available
- Anesthesia of the great toe more difficult and typically 3-sided/4-sided ring blocks [see belo].
Web-Space Block

It is the least painful of all and provides the right level of anesthesia.
- Prepare a sterile field [part preparation with betadine solution and sterile draping]
- Keep the hand of the patient with pal down.
- Keep the needle and syringe loaded with anesthetic just distal to metacarpal-phalangeal (MP) joint into the webspace.
- With a slow push inject the anesthetic in the dorsal aspect of the web space.
- Then, slowly advance the needle straight down toward the volar aspect of the web space and infiltrate the tissue of the web space.
- Keep a caution to avoid the piercing of the volar aspect of the web space.
- Now withdraw the needle and repeat the procedure on the web space on the other side of the of the involved digit.
This method is effective in toes also except the great toe.
Transthecal Block
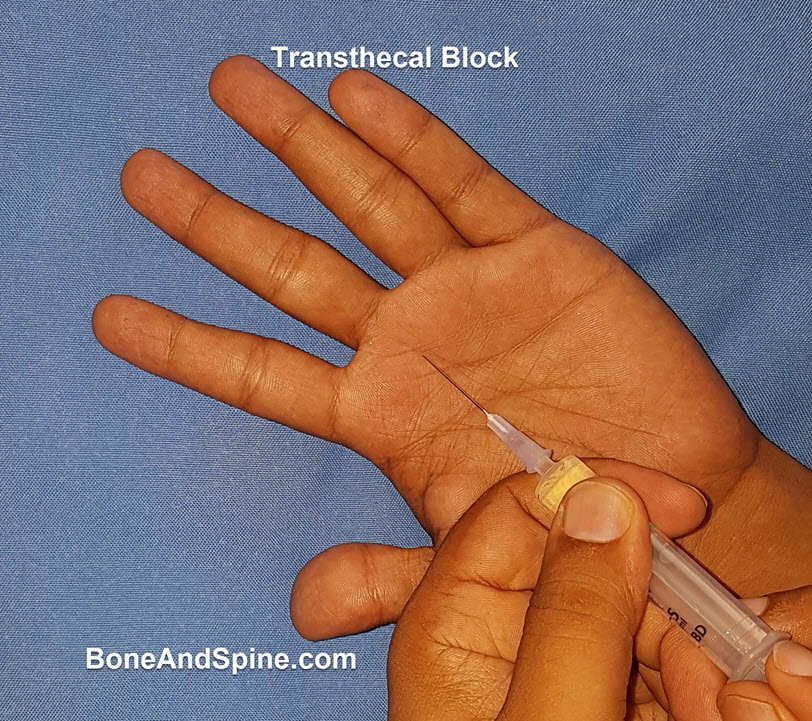
This is a quite effective block but bit painful because the space available for an anesthetic is less.
- Keep the patient’s hand on the sterile field with the palm up.
- Palpate the distal palmar crease and locate the flexor tendon sheath just distal to the palmar crease and insert the needle at a 45-degrees.
- Inject the anesthetic slowly. If there is a resistance, reposition the needle by slowly withdrawing it.
A modified version of this technique inserts the needle at a 90-degree angle at the metacarpal crease until the bone is hit. The anesthetic is injected after slowly withdrawing the needle.
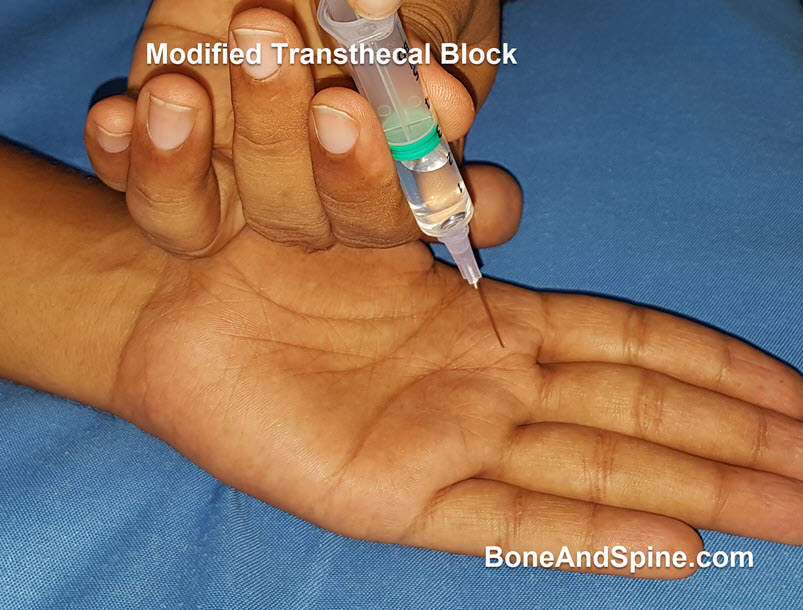
Use the other hand to keep the pressure just proximal to the injection site so that the flow is directed distally.
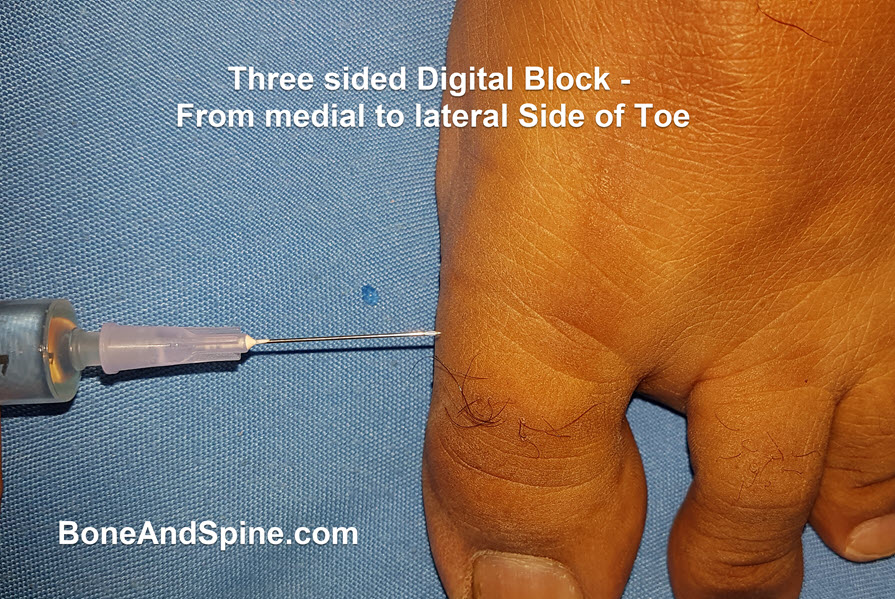
Three-Sided Digital Block
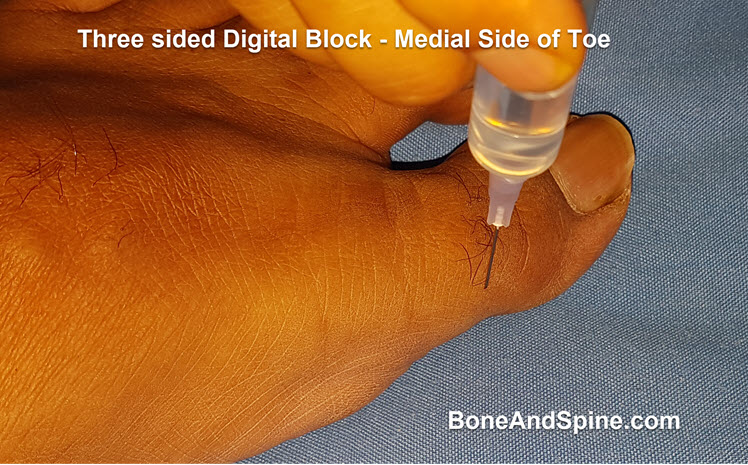
Though this anesthesia can be used for any digit, it is typically used in case of the great toe.
- Place the patient’s foot on a surface in a sterile field with sole touching the surface.
- For three-sided block
- Insert the needle at a 90-degree angle at the medial aspect of the digit, just distal to the metatarsal-phalangeal joint and inject the anesthetic as the needle is advanced toward the plantar side. Take care not to pierce the plantar skin
- Slowly withdraw the needle, redirect it medially and advance from medial to lateral side while injecting the anesthetic.
- Withdraw the needle and inject on the lateral side of toe in a similar fashion to the medial side

Four-Sided Ring Block
It is an extension of 3 sided block.
After completion of the above three steps, the needle is inserted at the lateral aspect of the digit on the plantar side and advance it medically as the anesthetic is slowly injected. This method is not preferred because of the risk of ischemic complications.
Wing Block Procedure
It is used when the distal part of the digit is affected, such as an injury to nail.
- Keep the hand/foot placed on the surface with the volar/plantar side down.
- With needle perpendicular to the long axis of the digit and at 45 degrees to the horizontal plane, insert the needle 3 mm proximal to an imaginary point where extensions of the lateral and proximal nail folds intersect
- Inject the anesthetic along the proximal nail fold and inject
- Slowly withdraw the needle and redirect it toward the lateral nail fold.
- If required, perform the procedure on the opposite side of the nail as necessary.
The method is not used very commonly. It is more painful than web space digital block