Last Updated on July 16, 2019
While the terms gait and walking are often used interchangeably, the word gait refers to the manner or of walking, rather than the actual walking process.
When we walk, we make the use of our two legs, alternately, to provide both support and propulsion, with at least one foot being in contact with the ground at all times. An individual’s style or way of walking – may change slightly with mood.
The gait cycle is the time interval between the exact same repetitive events of walking that generally begin when one foot contacts the ground [though ideally gait cycle can be considered from any position of the foot during walking].
To elaborate, if we consider beginning from right foot contacting the ground, it would be followed by lifting left foot off and thrusting it forward where it touches the ground. As the left foot is touching the ground, right foot is getting off the ground and is thrust forward and contacts the ground again.
The time when the right foot contacts the ground to the time when it contacts again constitutes one gait cycle.
It refers to all activity that occurs between two successive heel contacts of the same foot. As noted before, it is broken up into stance phase and swing phase.
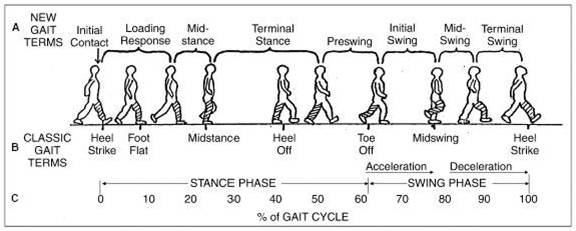
Stance Phase of Gait Cycle
The stance phase is part of the gait cycle that occurs when the foot is in contact with the ground. It begins with heel strike and ends with toe off of the same foot. Stance phase accounts for accounts for 60% of the gait cycle.
Stance has several phases
- Heel strike
- Foot flat
- Mid-stance
- Heel off
- Toe off
Heel Strike
It starts when the heel comes in contact with the floor. The ankle is in a neutral position, the knee is slightly flexed and hip is approximately in 30 degrees of flexion.
With heel strike, body weight begins to shift onto stance limb.
Foot Flat
In this, the entire foot is in contact with the floor. The ankle moves into approx. 5-10 degrees of plantar flexion and knee moves into 15 degrees of flexion. the hip moves into extension allowing trunk and body to catch up to the limb. The weight of the body continues to shift on the stance limb.
Mid Stance
It is the point at which the body passes over the stance limb and where the leg is approaching the vertical position offering single-limb support with the other limb freely swinging forward.
The ankle moves into slight dorsiflexion, knee extends and hip continues to extend. The trunk is in the neutral position of rotation and arms are parallel to the body.
Heel Off
Heel off occurs when the heel just begins to lift off the floor. The ankle is in dorsiflexion initially and then in plantar flexion. The knee is extended and prepares to flex, hip is in hyperextension and trunk rotates to the same side.
Toe Off
It is a time in gait cycle when toes just leave the floor to when the toes leave the floor. Simultaneously, the opposite foot is in foot flat phase. It is the end of the stance phase and the beginning of the swing phase. Toes go into hyperextension and ankle begins to plantar flex and knee keeps moving to flexion. By end of this phase, the hip starts flexing.
Swing Phase of Gait Cycle
It is part of the gait cycle when the foot is not in contact with the ground. It begins when the foot leaves the floor and ends with the heel strike of the same foot and accounts for accounts for 40% of the gait cycle. It is nonweight bearing phase of gait. and consists of the following phases.
- Acceleration
- Mid-swing
- Deceleration
Acceleration
In the acceleration phase, the limb is behind the body and moving to catch up, ankle moves into dorsiflexion. Both knees and hip continue to flex.
Mid Swing
This phase involves the shortening of the limb to clear ground. The ankle is in a neutral position and knee in maximum flexion. Hip continues to flex.
Deceleration
Deceleration is last of swing phase. In this, the ankle is maintained in neutral, preparing for heel strike and knee moves to an almost full extension while the hip is in flexion.
Double Support and Single Support
Double support is the period in the gait cycle when both feet are in contact with the floor. It occurs when one limb is ending the stance phase and the opposite limb begins stance phase. About 10 percent of the gait cycle is spent in double support and it changes with speed. Faster gait leads to less double support time and slower gait leads to more time in double support.
Single Support is a period when only one foot is in contact with the ground. There are two periods of single support, right stance and left stance and
In running there is a period when none of the foot is on the ground. It is called nonsupport and this differentiates running from walking as nonsupport does not occur in walking.
Stride Length, Step and Cadence
Stride length is the distance traveled in one stride i.e. between two consecutive heel strike of the same foot. The step is the period covered between heel strike of one foot to heel strike of opposite foot.
Step length is the distance covered between heel strike of one limb and heel strike of the other limb.
Step Width is the distance by which feet are apart during walking. For measurement purpose, the distance between the heel centers of two consecutive foot contacts is taken as step width. Normally it is 2 – 4 inches
Cadence is the number of steps taken per minute and varies with walking speed.
Here is a video on the gait cycle.
Other Associated Movements
Center of gravity is highest at mid-stance, lowest at heel strike and the movement in normal course is about 2 inches.
Horizontal Displacement of center of gravity is side to side shift and is maximum at the time of single support phase of mid-stance. It is also about 2-4 inches.
Lateral pelvic tilt occurs when the weight is taken off the limb at toe off. In this hip abductors on contra-lateral side work to keep pelvis level.
Arms swing occurs in opposition to trunk rotation to control the amount of trunk rotation by providing counter-rotation
Normal Gait Variations
Child
A child walks with a wider base, faster cadence, and shorter stride length. Initial contact with the floor is with a flat foot and knees remain mostly extended during the stance phase.
Elderly
Elderly walk slower, spend more time in stance phase. There are longer periods of double support, shorter steps, less vertical displacement, and greater horizontal displacement.
Foot Pronation Pattern
Neutral Pronation
Neutral pronation is the normal amount of pronation when the weight distributes fairly evenly among all of the toes with a slight emphasis on the big toe and second toe.
Overpronation
This pattern causes the push off almost completely from the big toe and second toe. Tibia vara of 10 degrees, forefoot varus, leg length discrepancy, ligamentous laxity, or tight or weak gastrocnemius and soleus muscles have been associated with overpronation of the foot.
Supination
The weight of the body isn’t transferred at all to the big toe, forcing the outside of the foot to bear the load.
Image Credit
Physio-pedia
Abnormalities of Gait
Trendelenburg Gait
Trendelenburg gait occurs due to the weakness of the abduction mechanism of the hip especially weakness of gluteus medius muscle. It is also called abduction lurch gait. The patient lurches his trunk towards the affected side as due to the weakness of abduction mechanism the affected side is unable to lift opposite pelvis required for ground clearance of the opposite limb.
The patient lurches on the affected side for ground clearance of the opposite limb.
When a patient has bilateral Trendlenberg lurch [the lurch is on both sides], it is called Waddling Gait. It is seen in bilateral congenital hip dysplasia.
Antalgic Gait
Antalgic gait occurs due to pain in the affected side. The patient has reduced stance phase and winces with pain every time load is borne on the affected limb. The patient walks with a short shuffling gait.
Stiff Hip Gait
It is seen in patients of stiff hip and often is seen with abduction deformity of the hip. Because hip cannot flex, to clear the ground, the patient needs to sway to opposite side. Some compensation is offered by spine extension too.
Short Leg Gait
In short leg gait or short limb gait, the patient walks with a dip towards the affected side and can be gauged by pelvis dip and watching shoulder levels. The stance phase is almost equal on both sides.
Stiff Knee Gait
In this, the patient does not bend his knee and is seen in knee ankylosis or spastic paralysis. There is not enough flexion at the knee during swing phase and patient raises his pelvis so as to sweep off the heel during swing phase. There is no movement at his both knee joint. Think about a minute how such patient passes his stool. All movements at knee joint are restricted.
Gait in Neurological Disorders
In addition, following are seen in neurological disorders, especially in post polio residual paralysis
- Flat foot gait
- Hand to knee or thigh gait
- High Step or Foot Drop Gait [also seen in peroneal nerve palsy]
- Calcaneus or Peg gait