Last Updated on August 2, 2019
Dupuytren contracture is a thickening of the fibrous tissue layer underneath the skin of the palm [fibromatosis] and fingers leading to painless thickening and tightening (contracture) of this fibrous tissue which causes fingers to flex.
It is also known by the names of morbus Dupuytren, Viking disease or Celtic hand. It is named after surgeon Baron Guillaume Dupuytren.
Dupuytren disease is often used synonymously with Dupuytren contracture but there is difference between the two.
Dupuytren disease is a generalized disease that doesn’t only affect the palms of the hands. People with involvement may have
- Garrod pads – nodules on the back of knuckles [also called dorsal Dupuytren nodules]
- Ledderhose disease – and lumps in the arch of the feet (
- Nodules at the volar wrist crease
- Frozen shoulder (adhesive capsulitis of shoulder)
- Peyronie disease of the penis
- Increased risk of some malignancies types of cancer, and the risk of early death, but more research is needed to clarify these relationships.
But the exact and clear relation between above entities is not known yet.
The ring finger and little finger are the fingers most commonly affected, but any and all digits may be involved.
Dupuytren contracture is found more in people > 4o years old.
Men are more affected than women. Beyond the age of 80, it equally affects males and females. Patients must have realistic expectations that surgery can relieve some disability but that it cannot cure Dupuytren disease. Discuss all potential complications of the procedure, including complex regional pain syndrome. In addition, intensive rehabilitation with an occupational therapist is necessary postoperatively for an optimal outcome.
Relevant Anatomy
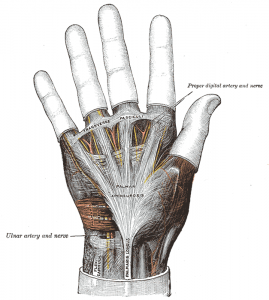
In the normal hand, the palmar aponeurosis runs longitudinally from the wrist, crosses over the superficial transverse palmar ligament, and splits into pretendinous bands to each digit. See the image below.
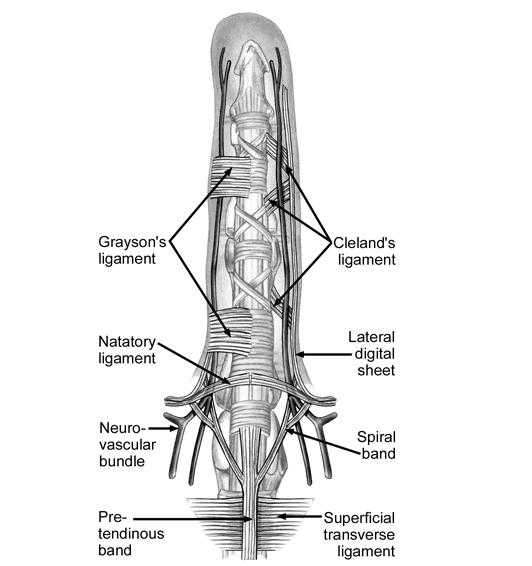
In the distal palm and fingers, the following superficial fascial components are typically involved in Dupuytren disease [see the image below for details]
- Pretendinous band
- Spiral band
- Lateral digital sheet
- Grayson ligament
- Natatory ligament
Pathogenesis and Cause of Dupuytren Contracture
Exact cause of Dupuytren’s contracture is not known though there are many theories. Following risk factors are suggested
- Genetic predisposition
- Alcoholism
- Diabetes
- Epilepsy
- Lung disease
- Smoking
Histology of the condition shows characteristics of hypertrophic scar formation.
There are three stages of Dupuytren contracture
- Proliferative stage: Intense cellularity with random collagen fibrils
- Involution stage: Collagen fibrils are organized along lines of tension. Myofibroblast is the predominant cell and aggregates near the collagen fibrils
- Residual stage: Uniformly oriented collagen, fibrosis is present and there are only a few cells.
In all stages, a core of type I collagen is surrounded by type III collagen.
Clinical Presentation of Dupuytren Contracture
Patients complain of knot or nodule or thickening on the distal palm or proximal palmar surface of the digits. The thickening may be noted long after its formation and is very slow to progress.
Ring finger is most commonly affected. Bilateral occurrences are known.
Pain is almost never a complaint unless nerve compression or tenosynovitis is present which can cause pain.
Tenosynovitis can develop and lead to pain when the nodules are large.
Flexion deformity develops with time and the patient reports an inability to straighten the fingers and perform tasks like grasping objects and typing.
A detailed history should be obtained to assess the presence of risk factors.
Examination reveals firm nodules that may be tender on palpation. The nodules are closely adherent to the skin and do not move with movement of finger [differentiation from nodule in tendon]
There is a presence of painless cords proximal to the nodules. There might be atrophic grooves or pits in the skin.
In late cases, metacrpophalangeal and proximal interphalangeal joint contractures may be present.
Other features of Dupuytren disease, as mentioned may be present.
Clinical Grades of severity
- Grade 1 – Thickened nodule and band in the palmar aponeurosis; may have associated skin abnormalities
- Grade 2 – Development of pretendinous and digital cords with a limitation of finger extension
- Grade 3 – Presence of flexion contracture
Differential Diagnoses
- Trigger finger
- Stenosing tenosynovitis with nodule
- Diabetic cheiropathy [changes in hand due to diabetes]
- Soft tissue tumor
-
- Epithelioid sarcoma
- Fibroma
- Giant cell tumor
- Lipoma
- Neurofibroma
- Palmar fibromatosis
- Palmar tendinitis
- Tophi
- Traumatic scars
- Ganglion cyst
- Camptodactyly
Lab Studies
No lab tests are required for making the diagnosis. Blood glucose levels may be done to know diabetic status.
Imaging
Xrays are normal.
Ultrasonography may reveal thickening of palmar fascia and nodule.
Treatment of Dupuytren Contracture
Dupuytren contracture has very slow progression and is not troublesome for years. Moreover, it may never progress in some cases.
Observation
Observation is a treatment choice in patients with nonprogressive, painless contracture and no functional impairment. These patients typically have mild disease and may be monitored every 12 months.
Non-operative Treatment
Conservative treatment consists of following options
Physical and occupational therapy
- Stretching with the application of heat and ultrasonographic
- Custom splint or brace to stretch the fingers further
- Range of motion exercises should be performed several times a day.
These measures can also be used after the surgery if the patient undergoes surgical correction of the contracture, physical therapy often is involved following the procedure
Enzyme Injection
Collagenase extracted from C histolyticum weakens and dissolves the Dupuytren cord.
It is a protease that hydrolyzes collagen and breaks down its triple helix conformation, thus disrupting the Dupuytren cord.
It results in enzymatic disruption of the cord. Injection is indicated for Dupuytren contracture with a palpable cord.
Corticosteroid Injection
Intralesional steroid injections [triamcinolone] can help in subjective improvement but could be associated with complications of steroid injections
Radiotherapy
It is effective in early disease and slows the progression. Radiotherapy is not effective in advanced disease.
Drugs
5-Fluoruracil decreases collagen production by fibroblasts and inhibit fibroblast proliferation and myofibroblast differentiation. It may be useful as an adjuvant therapy to surgery.
Surgery for Dupuytren Contracture
Surgery aims at excision of diseased to prevent progression of the disease.
Surgery should be considered in patients with metacarpophalangeal contracture more 30º or if there is any contracture of the proximal interphalangeal joint.
Metacarpophalangeal enzyme involvement is more amenable to surgical correction than proximal interphalangeal joint involvement.
Needling/closed Fasciotomy
Needle aponeurotomy new procedure which is less invasive and can be done under local anesthesia. It uses hypodermic needle to divide the diseased tissue. No incision is required. Early results appear equivalent to surgery, but long-term results are not known.
Needle fasciotomy may be an effective initial intervention in the treatment of Dupuytren contracture either alone or as a first step to subsequent.
Open Fasciotomy
It is sometimes used to manage more severe cases of Dupuytren contracture and it is also an outpatient procedure.
Fasciotomy is usually most successful for metacarpophalangeal flexion contracture.
Fasciectomy
Fasciectomy is a removal of fascial tissue. This could be regional (or selective) fasciectomy which removes only the fascia that is grossly affected. Extensive or radical fasciectomy is the excision of the entire palmar fascia, including tissue that appears grossly healthy.
Dermofasciectomy removes the diseased fascia and the overlying skin. It is usually reserved for patients with recurrent or severe disease.
Amputation
Amputation may be recommended if digital contracture is greater than 90º or if a vascular compromise has developed.
References
- Verheyden CN. The history of Dupuytren’s contracture. Clin Plast Surg. 1983 Oct. 10(4):619-25.
- Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase clostridium histolyticum for Dupuytren’s contracture. N Engl J Med. 2009 Sep 3. 361(10):968-79.
- Geoghegan JM, Forbes J, Clark DI, Smith C, Hubbard R. Dupuytren’s Disease Risk Factors. J Hand Surg. 2004/10. 29B:423-426.
- Trojian TH, Chu SM. Dupuytren’s disease: diagnosis and treatment. Am Fam Physician. 2007 Jul 1. 76(1):86-9.
- Strickland JW, Leibovic SJ. Anatomy and pathogenesis of the digital cords and nodules. Hand Clin. 1991 Nov. 7(4):645-57; discussion 659-60.
- Gosset J. Dupuytren’s disease and the anatomy of the palmodigital aponeurosis. Hueston JT, Tubiana R. Dupuytren’s Disease. London: Churchill, Livingstone; 1985. 13-16.
- Rayan GM. Nonoperative treatment of Dupuytren’s disease. J Hand Surg Am. 2008 Sep. 33(7):1208-10.
- Ketchum LD, Donahue TK. The injection of nodules of Dupuytren’s disease with triamcinolone acetonide. J Hand Surg Am. 2000 Nov. 25(6):1157-62.
- Hurst LC, Badalamente MA. Nonoperative treatment of Dupuytren’s disease. Hand Clin. 1999 Feb. 15(1):97-107, vii.
- Warren RF. The pathology of Dupuytren’s contracture. Br J Plast Surg. 1953 Oct. 6(3):224-30.
- Hnanicek J, Cimburova M, Putova I, et al. Lack of association of iron metabolism and Dupuytren’s disease. J Eur Acad Dermatol Venereol. 2008 Apr. 22(4):476-80. .
- Anwar MU, Al Ghazal SK, Boome RS. Results of surgical treatment of Dupuytren’s disease in women: a review of 109 consecutive patients. J Hand Surg Am. 2007 Nov. 32(9):1423-8.
- Watt AJ, Curtin CM, Hentz VR. Collagenase injection as nonsurgical treatment of Dupuytren’s disease: 8-year follow-up. J Hand Surg Am. 2010 Apr. 35(4):534-9, 539.e1..