Last Updated on August 29, 2021
Enneking Staging System and TGNM staging system are two main staging systems used for staging for benign and malignant tumors of the musculoskeletal system
Many factors are involved in choosing the proper therapy for the patients. They include the stage of the disease, the expected functional result after surgery, the age of the patient, the type of adjuvant therapy preoperative, whether or not therapy preoperative and postoperative, whether or not there is a pathological fracture and the patient’s wishes and his tolerance for risk-taking.
The Enneking surgical staging system
The Enneking surgical staging system has been used for classification of musculoskeletal tumors surgeons around the world. It is a reliable, reproducible, and has prognostic importance for musculoskeletal sarcomas, especially for those originating in the axial skeleton.
Enneking staging system is applicable only to mesenchymal malignancies.
In this system, there are separate staging systems for benign and malignant mesenchymal tumors.
Enneking Staging System for benign musculoskeletal tumors
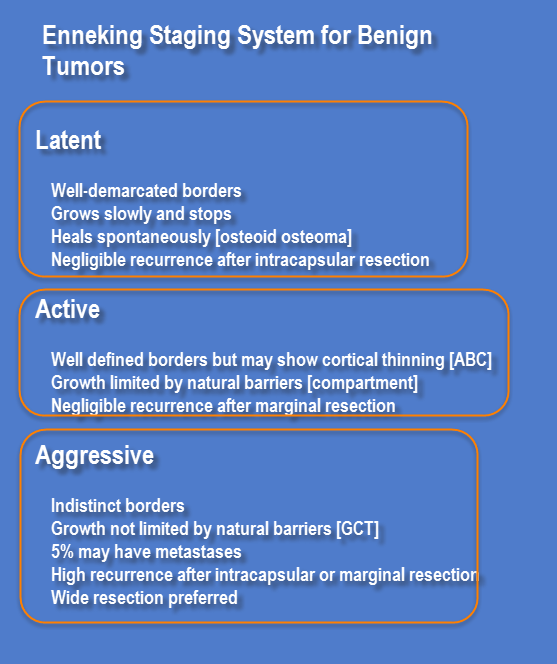
This classification is based on radiographic characteristics of the tumor-host margin. It consists of three categories: ie, latent, active, and aggressive.
If the lesion has well-demarcated borders, it is indicative of latent lesions.
An active lesion would show distinct borders because of permeation into host bone.
A more aggressive lesion would have even more indistinct borders.
Metastases are rare for locally aggressive benign lesions but do rarely occur in giant cell tumor and chondroblastoma.
| Stage | Description |
| Latent |
|
| Active |
|
| Aggressive |
|
Enneking surgical staging system for malignant mesenchymal tumors
Enneking surgical staging system for malignant mesenchymal tumors takes into account
- The surgical grade (G, G1, G2)
- Local extent (T, T1, T2)
- Presence or absence of metastasis (M0, M1)
There are three stages for malignant musculoskeletal tumors
Stage III represents any tumor with distant metastasis.
Stage II tumors are high grade and stage I are low grade
Stage I and II are further subdivided into two subcategories (A, B) based on the local extent of the tumor.
The stage of the tumor dictates the extent of surgical resection and margin.
Enneking staging for malignant musculoskeletal tumors based on surgical grade, local extent, and presence or absence of metastasis
| Stage | Grade | Site | Metastasis |
| IA | Low (G1) | Intracompartmental (T1) | No metastasis (M0) |
| IB | Low (G1) | Extracompartmental (T2) | No metastasis (M0) |
| IIA | High (G2) | Intracompartmental (T1) | No metastasis (M0) |
| IIB | High (G2) | Extracompartmental (T2) | No metastasis (M0) |
| III | Any (G) | Any (T) | Regional or distant metastasis (M1) |
Grades
In the Enneking staging system, a neoplasm is classified as either low (G1) or high (G2) grade.
Low grade – G1
- Low risk for distant spread (< 25%).
- Low mitotic rates
- Low nuclear to cytoplasmic ratio
- Limited pleomorphism.
High Grade – G2
- Higher incidence of metastasis
- Mitotic figures are seen on histology
- Prominent nucleoli
Local Extent
Local extent for any neoplasm refers to its containment in anatomic boundaries of a compartment.
Anatomical compartments have natural barriers, e. g. fascial septae muscle origins, etc. to prevent the extension of the tumor into adjacent compartments.
For example, a bone forms a compartment in itself. This compartment extends to the articular cartilage, cortical bone and its investing periosteum.
Joints are also compartments with their surgical boundaries being the articular cartilage and the joint capsule.
Throughout the body, there are many soft tissue compartments, e.g. quadriceps, hamstrings, biceps, and triceps.
The adequacy of the surgical margin is determined by whether or not there is a barrier between the plane or resection and the tumor.
Thus local extent determines the approach for the surgical procedure and feasibility for desired surgical margins.
A localized tumor can be removed by a smaller margin. But a high-grade lesion is more likely to invade surrounding host tissue and may require the use of adjuvant therapies to eradicate tumor cells that would remain after surgical resection.
Metastasis
The last major determinant in the surgical staging system is whether or not the patient has metastases to s distant site or the regional lymph nodes[ stage III = metastatic disease].
The presence of metastatic disease denotes a poor prognosis.
Limitations of the Enneking surgical staging system
The Enneking surgical staging system is based on the natural evolution of mesenchymal tumors and thus is not applicable to tumors originating in either the marrow or reticuloendothelial system. These include lymphomas, multiple myeloma, plasmacytoma, Ewing’s sarcoma, other round cell neoplasms, and metastatic carcinomas. Lesions originating in the skull also behave differently and thus cannot be staged or classified using this system.
Tumor Resection Depending on Enneking Staging
Malignant Tumors
Stage IA
These tumors are treated with wide excision and are usually amenable to limb salvage procedures.
Stage IB
Such tumors may be treated with wide excision, but the choice between amputation and limb salvage depends on the estimated amount of residual tumor left behind after a limb salvage procedure.
Stage II
High grade, are usually extracompartmental, and have a significant risk for skip metastases. They usually are not amenable to limb salvage operations and require radical amputation or disarticulation. Those responsive to chemotherapy may be treated successfully using wide excision and adjuvant therapy.
Stage III
Tumors which are responsive to chemotherapy and may be treated with aggressive resection. Those that are not responsive to adjuvant therapy should be treated with palliative resection.
Benign tumors
- Stage 1 tumors – Intracapsular excision (or curettage) is adequate.
- Stage 2 tumors – Extracapsular excision passing through the reactive zone.
- Stage 3 tumors – Wide margins of resection are required in stage 3 lesions (aggressive benign tumors). In areas that are not amenable to wide excision, marginal excision together with adjuvant treatment (eg, radiation therapy).
TGNM Classification
The American Joint Committee for Cancer has proposed their own staging system for soft tissue sarcomas [ in contrast to bone sarcomas].
The AJCC staging follows a TGNM system
- T (tumor) refers to the size of the primary neoplasm
- G (grade) refers to the histopathologic grade
- N (nodes) refers to the presence of lymph node involvement
- M (metastasis) refers to the distant spread to other organs
Description of the TGNM system
| TGNM component | Description | |
| Primary tumor (T) | ||
| TX | Primary tumor cannot be assessed | |
| T0 | No evidence of primary tumor | |
| T1 | Tumor < or =5 cm | |
| T1a | Superficial tumor | |
| T1b | Deep tumor | |
| T2 | Tumor > 5 cm | |
| T1a | Superficial tumor | |
| T1b | Deep tumor | |
| Regional lymph nodes (N) | ||
| NX | Regional lymph nodes cannot be assessed | |
| N0 | No regional node metastasis | |
| N1 | Regional lymph node metastasis | |
| Distant metastasis (M) | ||
| MX | Distant metastasis cannot be assessed | |
| M0 | No distant metastasis | |
| M1 | Distant metastasis | |
| Histologic grade (G) | ||
| GX | Grade cannot be assessed | |
| G1 | Well-differentiated | |
| G2 | Moderately differentiated | |
| G3 | Poorly differentiated | |
| G4 | Dedifferentiated or anaplastic | |
As compared to Enneking, this system does not correlate well with surgical procedure due to lack of consideration to anatomic planes and compartments.