Last Updated on May 12, 2022
Types of Surgical resection of the musculoskeletal tumors depend on the stage of the tumor and the type of surgical margin dictated by the histological grade which is required for the definitive local control.
There are a number of modifying circumstances to be considered before the decision for surgery is made, e.g. the patient’ s age wishes and expectations, lifestyle and expected function after reconstruction.
In malignant musculoskeletal tumors, the surgery can be of two types
- Limb-sparing where a functional limb is preserved
- Amputation
Tumor and Its Surrounding
The tumor is surrounded by a reactive zone. pseudocapsule is formed by compression of tumor cells and fibrovascular zone of reactive tissue. This gives the tumor appearance of encapsulation. A pseudocapsule may have tumor cells within known as satellite or micrometastatic lesions. These are causes of the local recurrences.
Outside the pseudocapsule, if not breached, the normal tissue is found
Types of Surgical Resection of Tumors
Four types of surgical resection were classified by Enneking. The classification is dependent on the margin of the tissue resected.
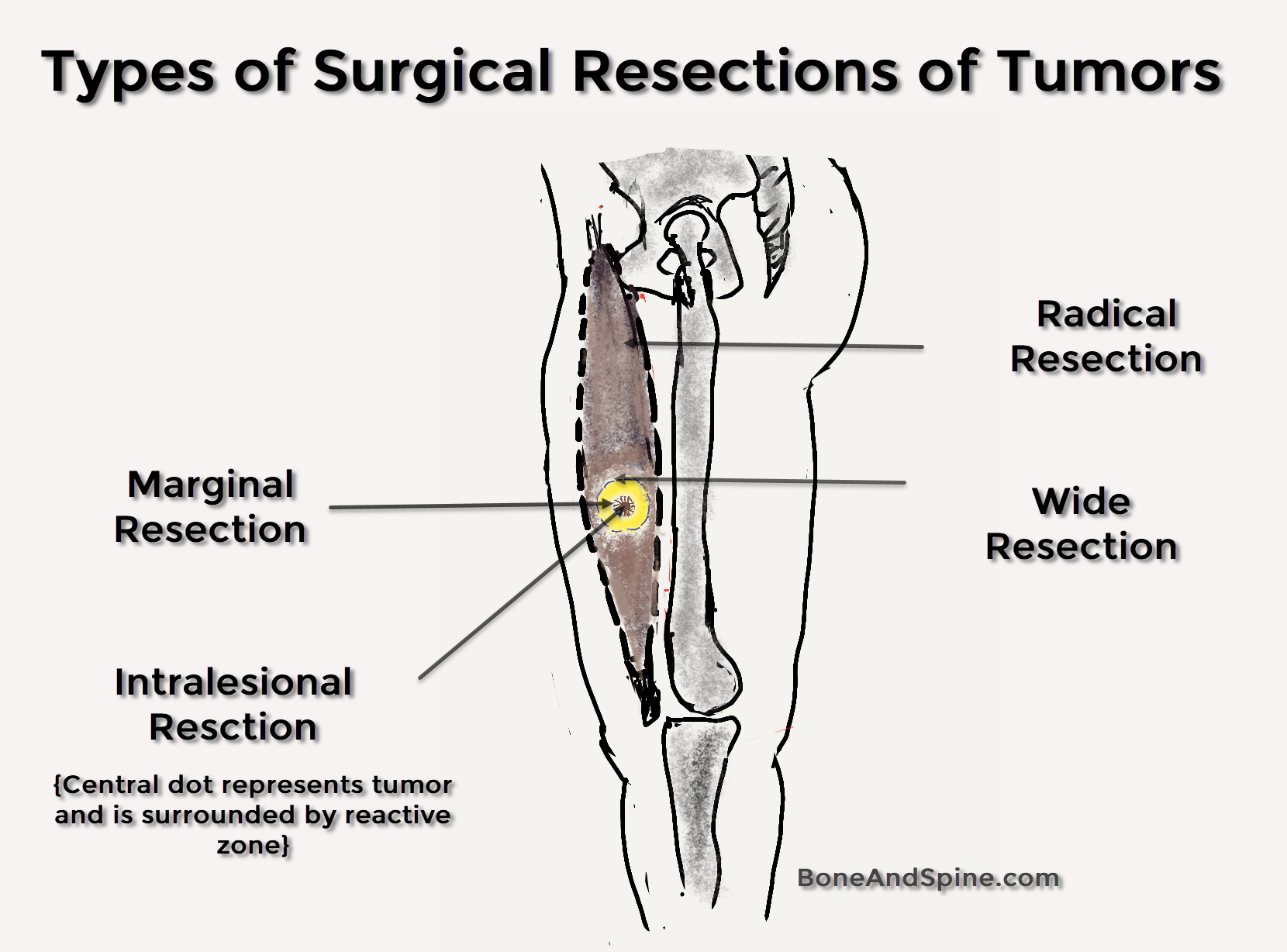
These are
- Intralesional margin
- Marginal Margin
- Wide Margin
- Radical Margin
We would discuss them one by one.
Read more about Enneking Staging System
Intralesional Resection
In this procedure, the tumor is actually entered and then removed piecemeal, leaving behind microscopic and macroscopic foci of tumor in both the tumor bed and the tissues bordering the surgical approach. It is considered in tumors like enchondromas, chondromyxoid fibromas, and benign osteoblastoma. It can be used in aggressive tumors by using adjuvant therapy along with resection.
Adjuvant therapy may consist of cryotherapy or other chemical agents. Liquid nitrogen is used in cryotherapy.
Adjuvant therapy aims to kill the microscopic and macroscopic foci of tumor left behind by intralesional resection. Curettage is an example of intralesional resection.
Curettage involves opening a window in the bone by removal of cortex and removal of tissue by scraping or scooping.
Intralesional excision with cryotherapy has been used in an increasing number of bone tumors such as ameloblastomas and aneurysmal bone cysts, low- and medium-grade chondrosarcoma and more recently central osteogenic sarcomas.
Giant cell tumors have been treated by cauterizing the tumor bed with phenol and filling the cavity with methylmethacrylate bone cement. The treatment with phenol extends the surgical margins and the filling of the defect with methylmethacrylate bone cement provides immediate support for the load-bearing bone. In addition, bone recurrences if they should occur, can be easily visualized at the margins of the cement. Phenol is not preferred as it is frequently hard to control and often causes chemical burns to nearby soft tissues.
The greatest use of intralesional excision for malignant disease is found in the treatment of pathological fractures caused by metastatic carcinomas. When combined with rigid internal fixation, and methylmethacrylate bone cement, it provides an excellent means for palliation and preservation of limb function.
Most of the intralesional removal of the tumor is planned but can also occur by amputation through the tumor.
Debulking is a type of intralesional resection where the aim is to reduce the size of the tumor. This is done when the tumor cannot be removed in toto and is usually followed by radiotherapy or other procedures.
Marginal Excision
This removes a lesion in one piece by dissecting along the pseudo-capsule or through the reactive tissue around the lesion. If done for malignant tumors, it leaves microscopic disease at the margin of the wound in a high percentage of the cases. Marginal excision is adequate for most benign tumors and a very few low-grade malignant tumors. In required cases, it is recommended to use radiotherapy to achieve tumor control, preserve the function of the limb and minimize the recurrence.
Wide Excision
The plane resection is entirely through the normal issue and away from the pseudo—capsule and the reactive zone around the tumor. There is no effort made to remove the entire compartment that contains the tumor. A wide amputation is an example.
Wide amputation has been the procedure of choice in many soft tissue sarcomas. The width of the margins, however, is controversial. Some surgeons recommend a margin of 5—8 cm when resecting soft tissue sarcomas. Other surgeons suggest narrower margin for low-grade sarcomas.
Radical Excision
Radical amputations and excisions are procedures in which the lesion, pseudo-capsule, reactive zone and the entire compartment involved are removed in one block. Most centers have now stopped using radical margins for all but a few extensive high-grade sarcomas. Local control can usually be achieved by a wide resection with or without adjuvant radiation therapy.
Tumor Resection Depending on Enneking Staging
Malignant Tumors
Stage IA
These tumors are treated with wide excision and are usually amenable to limb salvage procedures.
Stage IB
Such tumors may be treated with wide excision, but the choice between amputation and limb salvage depends on the estimated amount of residual tumor left behind after a limb salvage procedure.
Stage II
High grade, are usually extracompartmental, and have a significant risk for skip metastases. They usually are not amenable to limb salvage operations and require radical amputation or disarticulation. Those responsive to chemotherapy may be treated successfully using wide excision and adjuvant therapy.
Stage III
Tumors which are responsive to chemotherapy and may be treated with aggressive resection. Those that are not responsive to adjuvant therapy should be treated with palliative resection.
Benign tumors
- Stage 1 tumors – Intracapsular excision (or curettage) is adequate.
- Stage 2 tumors – Extracapsular excision passing through the reactive zone.
- Stage 3 tumors – Wide margins of resection are required in stage 3 lesions (aggressive benign tumors). In areas that are not amenable to wide excision, marginal excision together with adjuvant treatment (eg, radiation therapy).