Last Updated on April 8, 2022
Distal humerus fractures or distal third humerus fractures are fractures of the distal part of the humerus. It is an umbrella term for a group of injuries that may occur. Namely, the following constitute distal humerus fractures
- Fractures of lateral epicondyle
- Fractures of medial epicondyle
- Condylar fractures – lateral or medial condyle
- Intercondylar fractures
- Capitellem fracture
Intercondylar fractures are the most common type of injury in distal humerus fractures.
The overall incidence of distal humerus fracture in adults is 0.5% of all fractures and 30% of all . The nature of the injury is commonly severe and is often associated with injury to surrounding soft tissue and nerves.
[Note: This article mainly focuses on adult distal humerus injuries. Injuries to pediatric elbow are discussed in pediatric trauma section]
The outcome of the fractures around the elbow is determined by the anatomical part involved, by the degree of displacement, and by the degree of comminution.

Anatomy of Distal Humerus
The elbow has the capacity to flex and extend within the sagittal plane and also to rotate around a single axis. The Elbow joint consists of three different articulations, as follows:
- Radiocapitellar joint
- Olecranon-trochlear joint
- Proximal radioulnar joint
Motion within the sagittal plane occurs at the ulnohumeral articulation within the semilunar notch.
The distal end of the humerus is flattened, expanded transversely, and rounded at the end which presents articular and nonarticular surfaces.
The articular portion forms the elbow joint and articulates with the radius and ulna.
The posterior surface of the distal humerus is nonarticular which allows fixation on this aspect.
The distal humerus resembles a triangle, with the medial and lateral columns making up the sides and the trochlea forming the base. These columns are separated by a very thin layer of bone that posteriorly makes up the olecranon fossa and anteriorly composes the coronoid fossa. The lateral column ends distally in the capitellum.
The capitellum is the lateral convex portion of the lateral condyle which is covered on its anterior and inferior surfaces with articular cartilage. It articulates with the head of the radius. The medial column is entirely nonarticular.
The ulnar nerve lies just behind the medial epicondyle.
Few points to remember
- The lateral column lies in approximately 20° of valgus relative to the humeral shaft.
- The medial column is aligned at a 40° angle to the shaft and ends in the trochlea.
- The capitellum is angulated 30-40° anteriorly. The trochlea is angulated 25° anteriorly.
- The trochlea is larger in diameter medially than laterally and ends more distally than the capitellum in the coronal plane [This leads to a valgus position of the elbow in extension.]
The blood supply around the elbow is primarily fed by anastomotic vessels from the brachial artery.
The ulnar nerve and radial nerve are important nerves in relation to distal humerus fractures. The ulnar nerve is in the cubital tunnel just below the medial condyle and is often need to be exposed in surgeries for distal humeral fractures.
The radial nerve is in the spiral groove and runs between brachioradialis and brachialis. It divides into posterior interosseous nerve and superficial radial nerve before entering the forearm.
 Humerus bone widens distally in the coronal plane to a maximum between the medial and lateral epicondyles and narrows from proximal to distal in the sagittal plane before its distalmost articular segment expands and juts anteriorly.
Humerus bone widens distally in the coronal plane to a maximum between the medial and lateral epicondyles and narrows from proximal to distal in the sagittal plane before its distalmost articular segment expands and juts anteriorly.
This forms kind of lateral and medial column that diverge medial and lateral columns. At their most distal point, they are joined by the “tie arch,” consisting of the articular segment—the trochlea and the capitellum.
Important Muscles and Ligaments
Common flexor muscles (originate from medial epicondyle)
- Palmaris Longus
- Pronator teres
- lexor carpi radialis
- Flexor Digitorum Superficialis
- Flexor Carpi Ulnaris
Common extensors (originate from lateral epicondyle)
- Anconeus
- Extensor Carpi Radialis Longus
- Extensor Carpi Radialis Brevis
- Extensor digitorum
- Extensor Digiti Minimi
- Extensor Carpi Ulnaris
Important Ligaments
- Medial Collateral Ligament
- From distal medial epicondyle to sublime tubercle on ulna
- Primary restraint to valgus stress in range 30-120 degrees range of motion
- Becomes tight in pronation
- Lateral collateral ligament
- Originates from distal lateral epicondyle and inserts on crista supinatorus
- It stabilizes against posterolateral rotational instability
- Becomes tight in supination
Causes of Distal Humeral Fracture
The fracture typically occurs when there is a force applied to the upper limb when the joint is flexed more than 90 degrees.
The fracture either results from a motor vehicle accident or falls while walking.
In the elderly, the fracture is the result of low-energy falls whereas in younger patients high energy impact is needed to cause a fracture.
Associated injuries
In high energy settings,
- Elbow dislocation
- Terrible triad injury [Combination of radial head fracture, coronoid fracture, and elbow dislocation]
- Floating elbow [Fractures on both sides of the elbow. For example supracondylar fracture with radius ulna fracture]
Distal Humerus Fracture Classification
AO/OTA classification
- A type- Fracture is nonarticular.
- B Type- A partially articular fracture with articular fragments remaining in continuity with the shaft
- C Type- Articular fractures with no articular fragments remaining in continuity with the shaft
- C1: T or Y fractures
- C2: Articular fracture is simple, but the nonarticular supracondylar area is segmental or comminuted
- C3: Articular segment is segmental or comminuted.


Classification based on Columns
Supracondylar fractures
- Above the condylar area
- Generally transverse or oblique.
- Very common in children and are managed differently than adults
- Treatment in adults requires internal fixation and using two plates for fracture fixation.
Distal single column fractures
Milch further unclassified these fractures
- Milch Type I- Lateral trochlear ridge intact
- Milch Type II- Fracture through the lateral trochlear ridge
- Lateral condyle fractures are more common than medial
- Often require surgery
Bicolumnar fractures
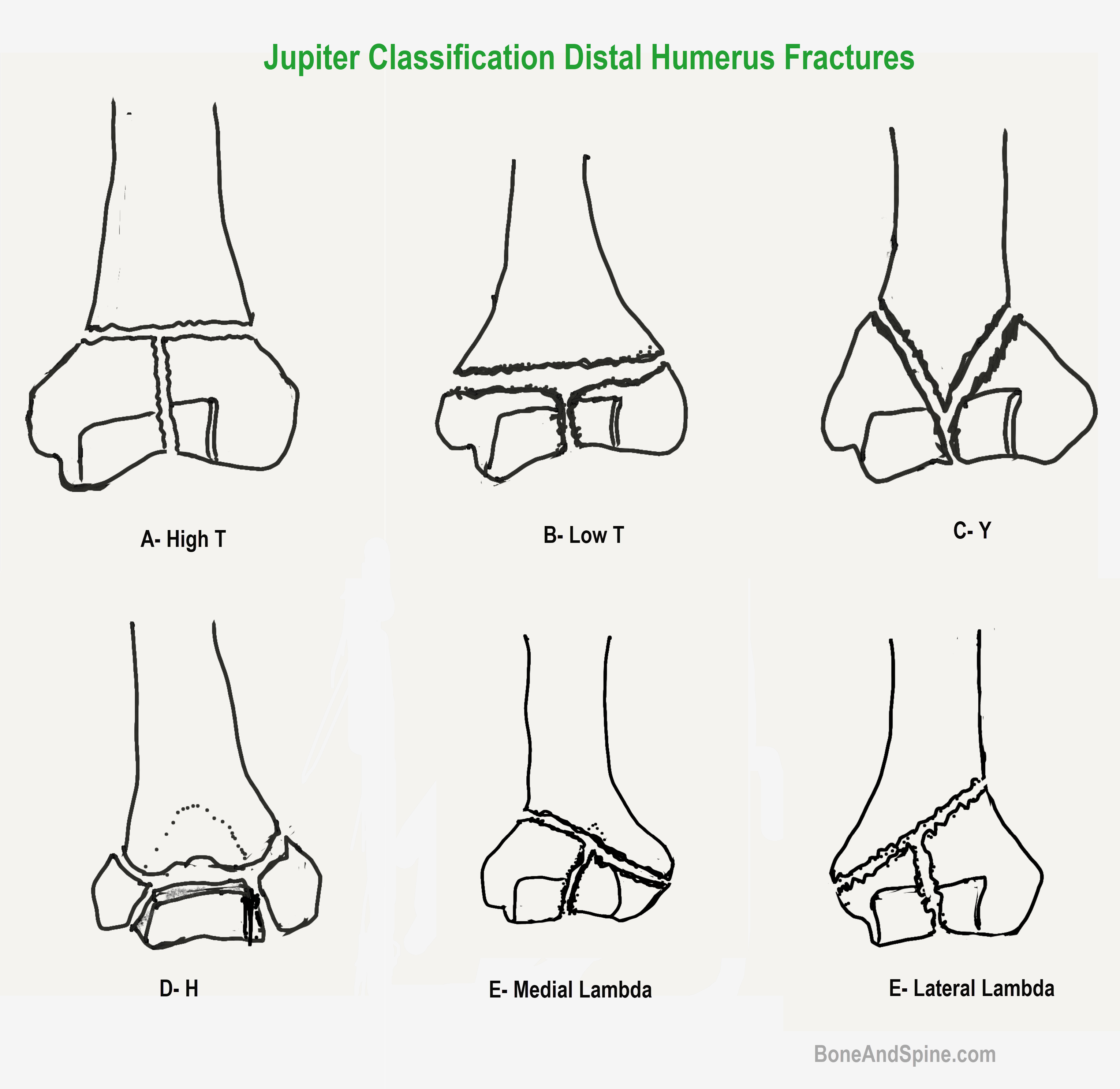
These are classified using Jupiter classification system. The classification is based on fracture pattern .
| Jupiter Classification of Two-Column Distal Humerus Fractures | |
| High-T | Transverse fracture proximal to or at upper olecranon fossa |
| Low-T | Transverse fracture just proximal to trochlea (common) |
| Y | Oblique fracture line through both columns with the distal vertical fracture line |
| H | Trochlea is a free fragment (risk of AVN) |
| Medial lambda | Proximal fracture line exists medially |
| Lateral lambda | Proximal fracture line exists laterally |
| Multiplane T | T type with an additional fracture in the coronal plane |
Classification based on Fragments Fractured
- Fracture of Lateral Epicondyle
- Fractures of the Medial Epicondyle
- Lateral Condyle Fractures
- Medial Condyle Fractures
- Capitellum Fractures
Classification Based on Plane of Fracture
- Coronal Shear Fractures [Fractures of the Capitellum]
- Sagittal Fractures
Clinical Presentation of Distal Humerus Fracture
Patients with a distal humerus fracture present with pain and swelling of the distal arm and elbow. Displaced fractures may cause a deformity and painful attempted movements.
Examination of the injured extremity and other associated injuries present should be done. With high-energy injuries, associated injuries to the head, chest, abdomen, spine, or pelvis must be excluded.
A complete examination of the neurovascular status of the extremity should be conducted.
In suspected vascular injuries Doppler studies or angiography should be performed.
The patient should be given an above-elbow splint after a thorough examination of the limb including neurovascular examination and x-rays. The limb should be checked for all the nerves.
If the distal pulses are absent, the limb should be monitored for vascular injury.
Imaging for Distal Humerus Fracture
X-ray
Recommended views are an anteroposterior and lateral view of the elbow. The entire length of the humerus and forearm should be recorded.




A wrist x-ray should be sought if there is a distal tenderness. A traction view may assist in surgical planning but CT is better.
CT
CT is performed in complex intraarticular fractures. 3D reconstruction of CT images helps to understand the fracture anatomy better.
MRI
MRI is not indicated in acute injury.
If there is an additional injury present, investigations might be needed accordingly. For example, an arteriogram for arterial injury.
Treatment of Distal Humerus Fractures
Factors That Affect The Treatment Decisions
- Age and Bone Quality
- Poor bone quality will make implant holding difficult
- Patient demands and goals
- Type of Fracture
- Fracture pattern
- Displacement
- Comminution
- joint involvement
- Open fractures
- Vascular injuries
- Associated bony injuries would always require internal fixation.
- Unsalvageable joint – Elbow replacement.
Non-Operative Treatment
Distal humerus fractures in adults are best treated with open reduction and internal fixation. This allows anatomic reduction and an early range of motion exercised.
Nonoperative treatment depends on the fracture type. Nonoperative treatment of fractures includes casting and immobilization. Undisplaced fractures especially extraarticular can be safely managed by casting and immobilization.
Following fractures can be managed conservatively
- Medial epicondylar fractures with less than 3 mm displacement
- Undisplaced lateral epicondylar fractures
Fractures with articular involvement, comminution, displacement, or both should not be treated with conservative means.
But in spite of indications, there could be circumstances where a patient is not suitable to get operative treatment. For example, debilitated patients, patients with other ailments that make them poor candidates for anesthesia, the problem with local sites such as degloving injuries
Such cases need to be treated non-operatively with cast immobilization or skeletal traction.
Surgical Management of Distal Humerus Fractures
Restoration of articular congruity, elbow stability and decreased risk of posttraumatic arthritis and elbow stiffness are the main goals of the surgery.
Main indications for surgery are
- Intra-articular fragment displacement
- Supracondylar comminution and displacement
- Open fractures
- Floating elbow patterns
- Neurovascular injury
- Compartment syndrome
- Multiple traumatic injuries
Closed reduction and percutaneous pinning
Closed reduction and percutaneous pinning is done mainly in children. It could be done in selected distal humerus fractures in adults.
Open reduction internal fixation
Most of the adult fractures require open reduction and internal fixation especially supracondylar humerus fractures and intercondylar fractures of the distal humerus.
Total elbow arthroplasty
It should be considered in elderly patients and non-salvageable distal humerus fractures.
Distal humerus fractures should be operated on as early as possible. Undue delay can cause elbow swelling which would interfere with tissue closure.
If the injury to soft tissues is severe to permit safe surgery, then definitive surgery should be delayed by immobilizing the fracture and bridging the elbow with an external fixator to allow some degree of reduction and maintain length.
Prognosis
The overall prognosis of the distal humerus fractures is good. Complex fractures are associated with a less favorable prognosis but with timely intervention results in a good functional elbow.
Open fractures, comminuted intra-articular fractures, and fractures with neurovascular injuries may result in less than optimal limb function.
Loss of terminal extension is frequently observed after distal humerus fracture. Chronic exertional pain can be observed in as many as 25% of patients who have suffered such injury.
References
- Jupiter JB, Mehne DK. Fractures of the distal humerus. Orthopedics. 1992 Jul. 15 (7):825-33. [
- Xie X, Qin H, Shen L, Zeng B, An Z. Open reduction and bi-columnar internal fixation of intra-articular distal humerus fractures through a combined medial and lateral approach. Eur J Orthop Surg Traumatol. 2014 Oct. 24 (7):1115-22.
- Barco R, Streubel PN, Morrey BF, Sanchez-Sotelo J. Total Elbow Arthroplasty for Distal Humeral Fractures: A Ten-Year-Minimum Follow-up Study. J Bone Joint Surg Am. 2017 Sep 20. 99 (18):1524-1531.