Last Updated on October 27, 2023
Popliteal artery entrapment syndrome refers to symptoms of claudication and leg ischemia due to compression of the popliteal artery due to congenital deformity of muscles, tendons or fibrous tissues. Compression of the popliteal artery decreases blood flow to the lower leg and can damage the artery. Popliteal artery syndrome was described first in 1879 by Anderson Stuart.
It occurs most often in athletes under age 30 [ patient age typically 25-40 years old], particularly those who are athletes [runners or play soccer, football or rugby] Males are affected more than females. As muscles grow in size, there is a greater chance of compression, a kind of over-use injury. [Also see functional popliteal artery syndrome below]
Less than 3% of people are born with a defect that can lead to popliteal artery entrapment syndrome, and most people with the condition never develop symptoms.
Pathophysiology
Popliteal artery entrapment syndrome usually occurs in younger patients who are healthier and more active than average for their age group, usually sportsmen requiring repeated sudden and forceful contraction of the calf which leads to hypertrophy of calf muscles. Drivers of heavy vehicles sit with a flexed knee and carry repeatedly alternating forced plantar extension with forced plantar flexion, which can result in calf-muscle hypertrophy.
Popliteal artery entrapment syndrome occurs when there is
- An abnormal anatomical relationship between the popliteal artery and the surrounding musculotendinous structures
- Hypertrophy of the musculotendinous structures
- Repeated arterial compression upon exercise.
Repeated trauma may lead to stenosis, complete artery occlusion or even formation of an aneurysm.
The anatomic anomalies may be seen in up to 3% of the population and are bilateral in about 60 percent of cases..
Arterial compression can result in chronic vascular microtrauma and local premature arteriosclerosis and thrombus formation resulting in distal ischemia, stenosis, and turbulent flow. There could be poststenotic ectasia [dilatation] or aneurysm formation.
Types of Anomalies
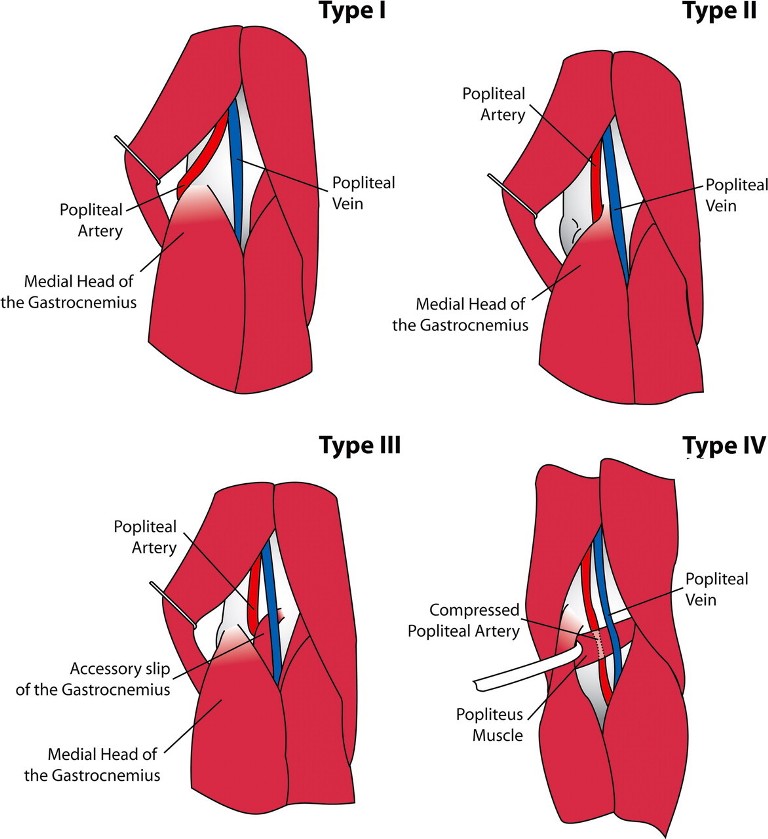
Type I
Medial head of the gastrocnemius is normal but the popliteal artery runs in an aberrant course around medial head around the medial head of gastrocnemius.
Type II
Medial head of the gastrocnemius is located laterally, no deviation of the popliteal artery. the artery passes medial and beneath the muscle
Type III
there is an abnormal muscle bundle from the medial head of the gastrocnemius that surrounds and constricts the popliteal artery
Type IV
Popliteal artery is entrapped by the popliteus muscle. artery lies deep in popliteal fossa entrapped by popliteus or fibrous band
Type V
The popliteal vein is entrapped with the popliteal artery in any of the above scenarios
Clinical Presentation of Popliteal Artery Entrapment Syndrome
Initially, when the artery is patent except during calf-muscle contraction, symptoms are limited to short periods of cramps or a feeling of coldness.
The onset of the symptoms is often sudden, during physical exercise. History of aching pain, numbness, and tiredness or cramping in the calf on exercise are typical symptoms which get relieved on rest. Leg swelling may be noted by some patients.
In the later stages, when the artery is affected by stable lesions (stenosis or occlusion, thrombus, or poststenotic aneurysm), symptoms of intermittent calf claudication occur.
[Pain in the leg on walking which is relieved by rest only is known as intermittent claudication.]
On physical examination, the posterior calf may be cooler than the rest of the body. Otherwise, the limb would appear normal. The pulses diminish with active foot plantar flexion or passive foot dorsiflexion revealing arterial compromise.
Acute ischemia due to blockage of a vessel may occur and is a surgical emergency. The patient presents with loss of circulation below the blockage because collaterals are not well developed.
Differential Diagnoses
- The cystic adventitial disease of the popliteal artery
- Thrombosed popliteal artery aneurysm
- Chronic exertional compartment syndrome
- Muscle strain
- Medial tibial stress syndrome
- Fibular and tibial stress fractures
- Nerve entrapment syndrome
- Referred pain from lumbar disc herniation
Imaging
Xrays
Radiographs are usually normal.
Doppler Ultrasound
Doppler is useful during the physical exam to detect changes in pulse when active plantar flexion or passive dorsiflexion is performed. The change is seen as an increase in peak velocity.
Computed Tomography
CT enables accurate grading of popliteal arterial stenoses and evaluation of surrounding muscular anomalies. It also tells about aberrant muscle and other tissue surrounding the artery, arterial diseases, and thrombosed popliteal artery aneurysms. Computed tomography can detect occlusion, deviation, and stenosis of the popliteal arteries.
CT can also confirm normal anatomy on the other leg.
Contrast Arteriography
It is considered to be a definitive test. The medial or lateral deviation and occlusion of the proximal popliteal artery with an extended knee confirm the diagnosis of popliteal entrapment. Complete obstruction of the popliteal artery in the presence of large collateral arteries and normal proximal and distal arteries is usually seen in the later stages of popliteal artery entrapment syndrome.
Even a slight irregularity of the vessel can indicate a degree of entrapment.
Arteriogram would also reveal stenosis [reduction of lumen size], obliteration of the lumen and post-stenotic dilation [part of the artery after stenosis dilates]
Digital Subtraction Angiography
Digital subtraction angiography [Digitally enhanced images of angiography] is well suited for the detection of slow flow and retrograde flow. It is able to tell about collaterals and helps in preoperative planning
MRI
MRI is the best imaging modality to demonstrate the underlying anatomic type of entrapment, which helps guide surgical management.
Treatment of Popliteal Artery Entrapment Syndrome
When the diagnosis of entrapment is made at an early stage and the popliteal artery is intact, the treatment of choice is the release of the popliteal artery by the division of the anomalous musculotendinous tissue.
When the popliteal artery is occluded, stenotic, or aneurysmal, the treatment of choice is vascular reconstruction, in addition to the division of the anomalous musculotendinous structure.
If decompression of the popliteal artery by the division of the anomalous muscle is not in itself adequate, the interposition of the autologous vein graft is also necessary. The graft is usually taken from the contralateral long saphenous vein.
Surgery brings good relief but the risk of re-entrapment could be as high as 30%. Calcitrant cases may require amputation.
Functional Popliteal artery entrapment syndrome
Functional popliteal artery entrapment syndrome is an uncommon overuse injury in young physically active with a similar presentation but no anatomic abnormality. Because of the absence of anatomic abnormality, this entity is often confused with chronic recurrent exertional compartment syndrome because the complaints are similar.
The major difference between the functional and anatomic entrapment syndrome is the absence of musculotendinous anomalies or vascular complications and the proportion of women affected.
In contrast to anatomical entrapment, functional popliteal artery syndrome is more common in young females.
Musculotendinous resection of soleus band and plantaris muscle is the treatment for this condition.
Image Credit
Wright et al. Popliteal Artery Disease: Diagnosis and Treatment, Radiographics March 2004 Volume 24, Issue 2