Last Updated on October 29, 2023
The iliotibial band is also called iliotibial tract and is a wide sheath of fibrous tissue that surrounds muscles on the lateral aspect of the thigh. It connects hip muscles to the tibia and plays an important part in thigh motion.
Origin, Course, and Insertion of Iliotibial Band
The iliotibial band is actually a thickening in the lateral part of the fascia lata, a deep fascia that completely ensheaths the thigh and is continuous with the strong lateral intermuscular septum, which is firmly anchored to the linea aspera of the femur. It also sends few fibers to the patellar retinacula.
The portion of the fascia lata attached to the front part of the iliac crest, and corresponding to the origin of the Tensor fasciae latae extends down the lateral side of the thigh as two layers, one superficial to and the other beneath this muscle; at the lower end of the muscle these two layers unite and form a strong band, having first received the insertion of the muscle. This band is continued downward as the iliotibial band.
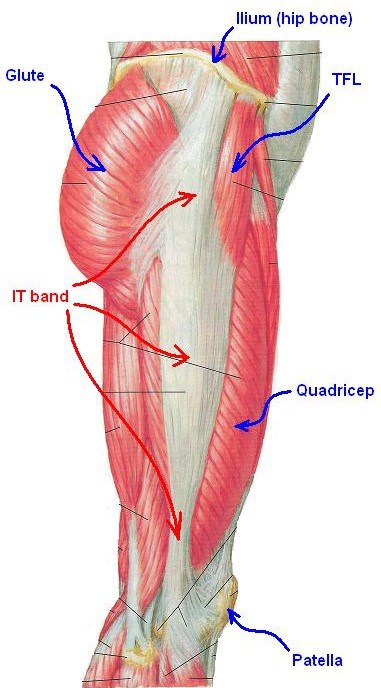
Thus, iliotibial band arises from the iliac crest, tensor fasciae latae and gluteus maximus muscles proximally travels along the lateral side of the thigh, sends some fibers to patellar retinacula at femoral epicondyle and inserts on Gerdy’s tubercle on the lateral aspect of the tibia.
The iliotibial band is also seen being consistently anchored to the femur in the region of the lateral epicondyle by obliquely oriented strong fibrous strands. Few authors claim that there is a tendinous part proximal to the lateral femoral epicondyle and a ligamentous part between the epicondyle and Gerdy’s tubercle making it a musculotendinous unit that starts at hip and inserts at the femur and a ligament that crosses the knee.
The iliotibial band is made of dense regular connective tissue and is extremely strong, tough, and avascular.
Histologically, it is composed exclusively of collagen fibers arranged in a regular pattern of straight lines making it very strong along the line of force. Some elastin proteins permit a degree of elasticity in the tissue.
Functions of Iliotibial Band
Functionally, the iliotibial tract extends the tensor fasciae latae muscle allowing it to function as an abductor, medial rotator and flexor of the thigh. It also allows the tensor fasciae latae and gluteus maximus muscles support and stabilizer of the knee while standing, walking, running and cycling etc.
Tensor fasciae latae is the muscle that originates from the outer lip of iliac crest, anterior border of the ilium and outer surface of the anterior superior iliac spine.
It inserts on the iliotibial band of fascia lata on the lateroanterior aspect of the thigh, which further inserts proximally into the lateral epicondyle of the femur then passes in its broad expansion between lateral aspect of the patella and finally inserts distally on Gerdy’s tubercle, on the lateral aspect of the tibia.
As noted before, tensor fasciae latae cause flexion, abduction, medial rotation of the hip and stabilizes the knee laterally.
Clinical Significance of Iliotibial Band
Iliotibial Band Syndrome
Iliotibial band syndrome is a condition caused probably by the friction of the tract moving across the tissues on the lateral side of the thigh.
The iliotibial band is not attached to the bone as it courses between the Gerdy tubercle and the lateral femoral epicondyle. This lack of attachment allows it to move anteriorly and posteriorly with knee flexion and extension. This movement has been hypothesized to cause the iliotibial to rub against the lateral femoral condyle, causing inflammation.
Another theory is that instead of friction, it is the compression of iliotibial band against a layer of innervated fat between the band and epicondyle that causes the problem.
This condition is common in runners and cyclists.
External Snapping Syndrome of the Hip
External snapping syndrome of the hip is caused by the thickened posterior border of iliotibial band or anterior border of gluteus maximus muscle near its insertion.
The iliotibial band is posterior to greater trochanter when the hip is extended and on flexion of it moves anterior to greater trochanter when the hip is flexed.
A tense iliotibial band may catch when it slides over superior margins of greater trochanter when hip flexed, adducted, or internally rotated.
However, the snapping may also occur from iliopsoas tendon catching over bony prominence at the lesser trochanter.
Contracture of the Iliotibial Band
contracture of the iliotibial band may occur in cerebral palsy and polio. The affected hip is brought into flexion, abduction and external rotation because of shortening of the iliotibial band.
Ober test is used to detect contracture of the iliotibial band. In this, the patient lies on normal hip, with affected hip and knee flexed. The hip is abducted and extended in order to center the iliotibial band on the greater trochanter. Now as there is an attempt to adduct the hip, the movement will be restricted because of the tightness of the iliotibial band.