Last Updated on October 29, 2023
Lower limb orthoses are advised for a variety of dysfunctions of the lower limb. Most of the lower limb orthoses use prefabricated components which are made of either stainless steel or aluminum. Stainless steel is more durable but aluminum is lighter.
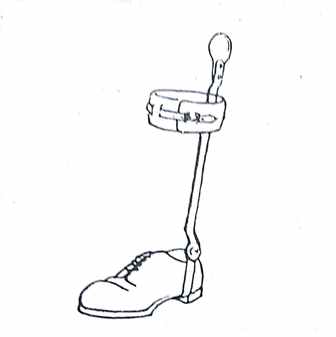
Below Knee Orthoses
Below knee orthosis has a primary function of controlling ankle joint. It usually consists of two uprights which are connected to a calf band and distally to a mechanical ankle joint. Most lower limb orthoses must be attached to shoes.
A sturdy shoe is an important component of the orthosis. The orthosis is attached to shoes by means of a stirrup, caliper or a shoe insert.
Shoe Attachments
Read more about shoe components
Stirrup
The stirrup is most commonly used method of attachment is a stirrup riveted directly to the sole of the shoe under the anterior section of the heel.
The solid stirrup encompasses the shoe like a U and becomes a permanent attachment between uprights and shoe. The stirrup may be employed with any type of ankle joint. It may be split at the bottom to permit shoe changes. This split p permits the accurate alignment of the mechanical joint with the anatomical joint but is heavier, thicker and less durable than solid one.
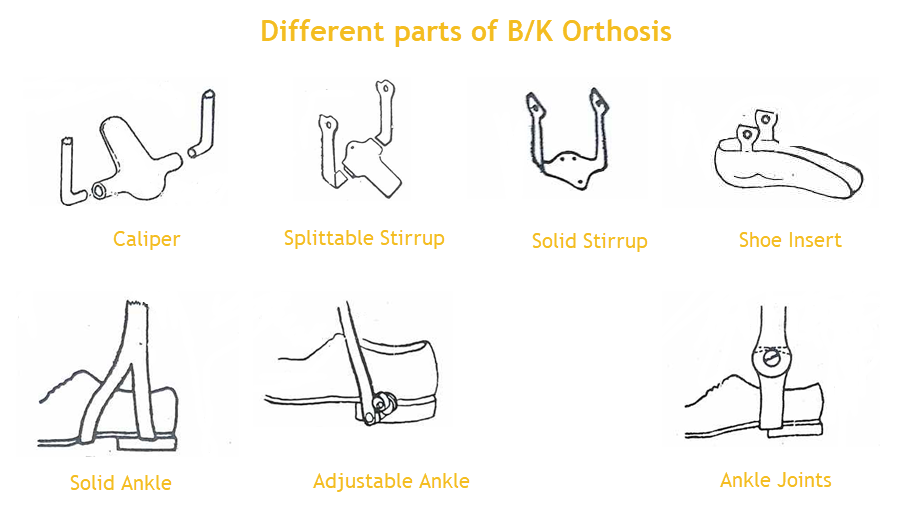
Caliper
Caliper is inserted into a tube placed in the heel of the shoe. It provides ease of interchangeability, minimal weight and facilitates fitting and adjustment.
The main drawback is that the mechanical ankle joint is at the level of the shoe heel which is considerably distal to the anatomical joint.
This incongruence between mechanical and anatomical joints will cause relative motion between the patient’s limb and orthosis.
Shoe Insert
The stirrup may be incorporated in a shoe insert which in turn fits into the shoe. This insert could be made of plastic, metal or metal with leather but plastic is more popular now because of the accuracy of fit.
The insert gives better control of the foot. The joints are well matched and the interchange of the shoes is simple. But it requires more skill and time and expensive.
Ankle Joints and Controls
Most of the mechanical ankles are single-axis joint which controls motion in the sagittal plane [dorsi and plantar flexion]. The ankle control may be in form of stops, assists or a solid ankle.
Ankle Joint Stop
Ankle joint stops may be set to allow for any predetermined degree of motion.
Posterior [plantar flexion stop] stop is often used in foot drop cases. It provides full dorsiflexion but limits plantar flexion.
An anterior stop would similarly restrict dorsiflexion while allowing plantarflexion. It is usually prescribed when the dorsiflexors are stronger than plantar flexors.
If the motion is to be restricted on both sides, it is accomplished by limited motion stop. It is indicated when a number of muscles around the ankle are involved.
Little or no motion may be achieved by not allowing any clearance between opposing surfaces of ankle joint.
In case of no restraint, a free ankle joint may be used. A free ankle joint permits full plantar and dorsiflexion while giving some control of lateral motion.
Adjustable Ankle Joint
IF the condition of the ankle joint is expected to change, then adjustable ankle joint, which allows the ankle to be readily set at different angles to accommodate the altered pattern may be employed.
This type of joint utilizes serrated interlocking discs to provide a clinically adjustable stop.
It is generally used as the positioning device to be worn during the night rather than to be worn during the day.
Solid Ankle
If rigid control of the ankle is desired, a solid ankle may be necessary. It is very strong but not adjustable.
Ankle Joint Assists
In contrast to stops which prevent motion, ankle joint assists may be utilized as an aid to weakened muscles. Motion at the ankle may be provided by the action of spring, elastic strap or the springiness of the material [plastic or wire] of which the orthosis is fabricated.
The spring-loaded dorsiflexion assist is an example of such an ankle joint. The action of spring helps to dorsiflex the foot during swing phase but allows controlled plantarflexion at heel strike.
A double action ankle assist helps both in dorsiflexion and plantar flexion.
AA wire-spring dorsiflexion assist accomplishes the motion by the recoil action of springy material but does not provide enough stability under great stress.
The use of assists is contraindicated in the presence of spasticity or when maximum control is required.
Double Axis Joint
Hitherto, single axis joints have been discussed.
A joint that assists motion in both the sagittal plane and frontal plane. However, the mechanical joint for other plane does not coincide with the subtalar joint and the addition of the second joint increases bulk of the orthosis.
Corrective Straps and Pads
These are used to provide additional control of the ankle in case the foot deviates medially or laterally.
This can be achieved by use of valgus or varus correction straps which attach to the shoe and buckle around opposite bars.
The side of the shoe to which strap is attached is dependent on the deviation. A medial placement of the strap would correct valgus condition.The padd might be added in case the force is considerable.
Uprights and Calf Bands
Uprights could be single bar [medial or lateral] which are more acceptable cosmetically or consist of two bars.
Single bars do not point as much stability as bilateral uprights.
Metal calf band with its leather cover secures the orthosis to the limb and provides a reaction point for the application of the force to the limb.
Torsion Shaft
A torsion shaft consists o tightly coiled spring within a flexible housing. With the upper end of the shaft attached to a well fitted pelvic belt and the lower end attached to the side of the shoe on to the lateral aspect of the calf band, the force developed by the spring can be used to apply a rotatory force to the limb.
This is useful in the management of spasticity and gait deviations like toe in or toe out.
Special Below Knee Orthoses
Patellar Tendon Bearing Orthosis
A patellar tendon bearing brim may replace a calf cuff if the reduction of weight transmission is desirable. It has the same contour as the proximal portion of a PTB socket and is designed to bear weight on the patellar tendon and tibial flares.
Little or no motion is allowed at the ankle joint, and therefore SACH heel and a rocker bottom are usually added to the shoe to provide better gait pattern.
A PTB brim is not indicated when there is impairment of a proximal portion of the leg.
Denis Browne Splint
This orthosis consists of two plates that are securely attached to infant shoes and then connected to a crossbar.
It is usually worn the whole day.
It can be used to hold feet in varying degrees of dorsiflexion and the hips in the abduction. The desired degree of rotation can be achieved by appropriate bending of the crossbar.
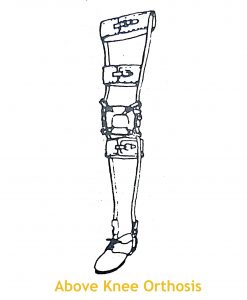
Above Knee Orthoses
The above knee orthoses may be used to support the body weight or prevent and correct abnormal motion at the knee. From knee down, the components are the same as of below knee orthoses except that the uprights extend upward to the knee joint.
Some type of knee pad is applied for further assistance in knee control.
The thigh uprights are shaped to the contour of the thigh and are held by one or two thigh bands.
A pelvic band and hip-joint may be added to the uprights.
Knee Joints
Because anatomical knee joint has a changing axis of rotation, mechanical joints which have fixed axis cannot move in complete unison with it. Therefore some shifting of the orthosis with respect to the limb occurs during flexion and extension of the knee.
This can be minimized by proper placement of mechanical knee joint.
Polycentric joints that accurately follow the natural knee have been devised. Changing the mechanical axis during flexion may aid in patient’s comfort when she sits
He joints discussed below are single axis joints.
Free Knee Joint
If the individual can control his knee against flexion but has a tendency toward mediolateral instability or recurvatum, a free knee joint may be used.
The free knee prevents recurvatum but allows for more natural gait than the locked knee.
Knee Locks
Drop ring lock is most commonly used knee lock. It is placed on the lateral bar but can be placed medially if the ipsilateral upper limb is involved too.
In full extension, the ring drops over the joint manually or by gravity. Spring loaded pull rod may be added that drives the drop lock down automatically so that individual need not bend to lock and unlock the joint.
An internal or plunger lock may also be used in place of the external lock. In this, when the knee is fully extended, the plunger snaps into a notch on the proximal end of the lower uprights and the knee joint is automatically locked
Cam lock is used in cases of severe spasticity. It consists of a spring-loaded, cam-shaped part which fits into a similarly shaped recess when the knee is extended.
The cam is maintained in the recess by spring in extended position. Because of curved surfaces, the cam locks are easier to release when forces are exerted. A bail, which is a type of lever is used to unlock both sides simultaneously.
A thigh release may be incorporated.
Adjustable Knee joint
An adjustable knee joint is particularly useful when a change in patient condition is anticipated. An example is the gradual stretching of knee flexion contracture.
A fan lock is an adjustable knee joint that incorporates a drop ring lock that maintains the desired knee position in standing and walking but unlocked to permit knee flexion when sitting.
Dial lock may be set to restrict flexion of extension but it permits free motion in the opposite direction. Since it is constructed with a long curved slot, the motion is restricted in one direction depending on the placement of the screw and allows free travel along the rest of the arc.
Offset Knee Joint
If the mechanical knee joint is placed posterior to the uprights, the knee will tend to extend when weight is transmitted through the bars.
In this way, the knee is stable without a lock during the stance phase and is free to bend during swing phase, allowing a more natural gait.
This type of knee joint cannot be used where there is knee flexion spasticity.
Knee Orthoses
Knee orthosis is prescribed when only mediolateral control of the knee is required.
It usually consists of two lateral bars with thigh and calf cuffs. Pads may be used to control knee alignment.
Hip Joints and Pelvic band
The movement of the anatomical hip joint may be controlled by attaching a hip joint and a pelvic band to the lateral uprights of the above knee orthosis.
Unilateral Pelvic Bands
The metal pelvic band encompasses the pelvis on the involved side below the iliac crest and above the greater trochanter and continues around the opposite side in form of a pelvic belt.
Bilateral Pelvic band
Each side of the bilateral pelvic band begins at a point just posterior to the anterior superior iliac spines, midway between the greater trochanter and the iliac crests.
It then curves downward and posteriorly to contact most prominent portion of the buttocks and continues slightly upward to overlie sacrum.
The proximal uprights of the hip joints attach to the pelvic band slightly anterior to the lateral midlines of the body.
Double Pelvic band
For maximum hip control, a double pelvic band may be used. But it is difficult to fit and requires making of a body cast.
Hip Joints
The pelvic band and lateral upright of the orthosis are connected by the hip joint. Most hip joints have a single axis, allowing for flexion and extension but limited hyperextension. The single axis hip joint may include a lock similar to those used in at the knee joint such as a drop lock or a cam lock, to prevent flexion while standing.
Two position hip locks provide a locking function at 90 degrees of the hip flexion and in full extension. These are useful in individuals who have difficulty in maintaining the sitting position because of muscle spasticity.
It controls abduction and adduction motion both in locked and unlocked position.
In cases where abduction and rotation control is desired, a double axis hip joint which allows for lateral motion in addition to flexion-extension may be used.
Any of the hip joints and pelvic bands may be used in various combinations.
Weight Bearing Devices
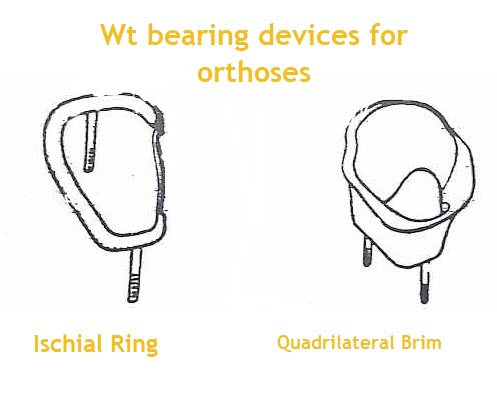
These devices play important role in a prosthesis for amputees and nonweight bearing limbs.
Weight-bearing devices can be provided in an orthosis by the use of an ischial ring or quadrilateral brim.
The ischial ring is simpler to fabricate but does not give as good as weight relief as does the quadrilateral brim since the weight bearing surface is quite small and there is little counterforce to maintain the ischial tuberosity on the ring.
A plastic laminated quadrilateral brim, designed with the same features as the proximal portion of a quadrilateral socket for amputees minimizes the problem presented by the ischial ring.
A patten bottom may be added to the orthosis with a quadrilateral brim so that foot does not touch the ground. The weight is transmitted by the orthosis from the orthosis to the patten bottom.
The ankle joint is eliminated and the lateral uprights which extend distal to the shoe are attached to the weight bearing bottom.
Torsion shaft used with Above Knee Orthosis
The torsion shaft may be used in conjunction with an above knee orthosis. It is used with a well-fitting pelvic band. It controls the rotation at the hips efficiently while allowing the freedom of other movements in all other directions.
Spinal Attachments
The spinal orthosis may be needed to control trunk motion in various neurological conditions.
These components are made from a material which is heavier and more rigid.
The pelvic band serves as a base for spinal orthoses.
The spinal orthosis consists of
Thoracic band
Extends below the inferior angles of the scapulae and ends midline of the rib cage
Uprights
Connects the pelvic and thoracic bands. A pair of posterior uprights is placed approximately two inches apart to avoid contact with vertebral spines. Lateral uprights if used, extend along the lateral midline of the torso.
Abdominal Support
It extends slightly below the xiphoid process of the sternum to slightly above the pubic symphysis. It covers the entire front of the abdomen and is fastened to the posterior or lateral uprights by at least three straps on each side.
In some cases, the support may be laced to lateral uprights, particularly when the orthosis is fabricated for heavy or obese individuals.