Last Updated on October 30, 2023
Kyphosis is a curvature of the spine which is to be present of the spine that causes curvature to be concave on the anterior side and convex on the posterior side. The reverse curvature is called lordosis.
Normal and Abnormal Curvatures of Spine
Kyphosis and lordosis are parts of normal spine curvature. In normal curvature of the spine cervical spine has lordosis, thoracic spine has kyphosis and lumbar spine has lordosis.
Sacral and coccygeal spines are also arranged in kyphotic curvature though these bone are fused and therefore, except trauma. The conditions causing the alteration of curvatures do not affect them.
But when it is said that somebody has kyphosis, it means there is a condition that causes abnormal forward bending of the spine.
Thus, kyphosis also denotes the excessive curvature or deformity of the spine [hyperkyphosis].
Kyphosis is also called round back or Kelso’s hunchback. It can result from degenerative diseases such as arthritis; developmental problems, most commonly Scheuermann’s disease; osteoporosis with compression fractures of the vertebrae, or trauma
The thoracic spine is mostly affected by kyphosis. For reference, normal kyphosis is defined as a Cobb angle of 20-40° measured from T2 to T12.
It is rare to see whole cervical or lumbar spine become kyphotic but angular kyphosis [the deformity includes few vertebrae only] could be seen either following trauma or instability of the spine.
Kyphotic abnormality can occur alone [the deformity is only in the sagittal plane] or can occur in association with scoliosis- an abnormality in the coronal plane.
When both the deformities are present, the entity is called kyphoscoliosis.
Kyphosis can cause pain in the back and has the potential to cause the neurologic deficit and affect functions of heart and lung by reducing space.

From side

From front

While most cases are mild, serious cases can be debilitating because high degrees of can cause severe pain and discomfort, breathing and digestion difficulties, cardiovascular irregularities, neurological problems.
Types of Kyphosis
It is mainly of two types – postural and structural
Postural Kyphosis is poor posture which leads to excessive rounding of the upper back. it is said to be present when exaggerated kyphosis is observed without finding any of wedging over three consecutive vertebral segments [as in Scheuermann kyphosis].
Muscular imbalance may play a role.
Postural kyphosis can be corrected by learning to remain in good posture.
The structural one is due to structural derangement in the spine. It is of two types – primary and secondary
Primary
Congenital and Scheuermann’s kyphosis are two further subtypes
Congenital
Congenital kyphosis is due to congenital defects in the spine.
Scheuermann’s kyphosis or Scheuermann’s Disease
This is a condition is generally presents in adolescent age group and occurs because the front of the spine doesn’t grow as fast as the back of the spine leading to rounding of the spine.
More on Scheuermann’s disease
Secondary Kyphosis
This develops as a result of some other pathology in the spine. Following conditions can cause this
- Connective tissue disorders
- Endocrine disease
- Infection
- Muscular dystrophy
- Neurofibromatosis
- Paget’s disease
- Polio
- Spina bifida
- Tumors
- Spondyloarthritis
- Degenerative Disc Disease
- Osteoporosis
- Post-laminectomy kyphosis
- Ankylosing spondylosis
- Compression fractures of spine and other trauma
Most of the secondary kyphosis occurs because pathological processes affect the integrity of anterior spinal column.
Clinical Presentation and Diagnosis
It must be emphasized that kyphosis is a finding on examination. Most of these patients could be asymptomatic.
In patients with symptomatic kyphosis, the complaint is often of the back pain. Some are concerned about the rounded look of the back.
A detailed history should be taken to rule out the possible causes.
In case of gait disturbances and other neurologic findings, a detailed workup would be necessary.
Routine lab workup includes CBC and routine biochemistry especially in patients with suspected pathology.
If the patient is considered for surgical correction, detailed workup including heart and lung functions should be done.
X-rays are basic imaging and play a crucial role in diagnoses and planning for management.
Upright posteroanterior and lateral images of the entire spine are most commonly used.
To find if kyphosis is present a plumb line is dropped from dropped from C7 on a full-length spine lateral view.
This line should pass through or just anterior to S1.
Normal kyphosis in thoracic spine is 20-40 degrees.
X-rays allow for quantification of the deformity which is done by measurement of Cobb’s angle.
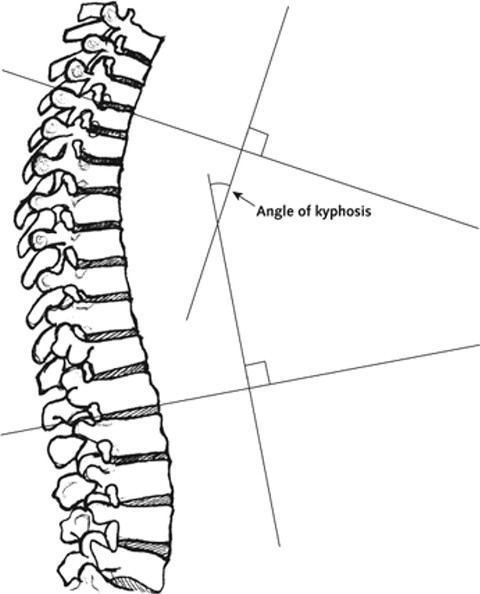
Cobb’s angle was originally created for measurement of scoliosis but now has been adapted for kyphosis too.
For determining the flexibility of the curve, the lateral x-rays are obtained with the patient in a supine position over a bolster.
[This information is important from surgical correction point of view. This information is useful in surgical planning. A flexible curve can be corrected on the table and then managed with posterior-only fusion. For stiff curves, anterior or combined anterior-posterior fusion is required.]
MRI can locate the neurological impingement and is important in surgical planning.
Bone density test before surgery can be considered to evaluate the fixation purchase issues.
Treatment
Most of the patients with kyphosis are not symptomatic and often require no treatment.
The treatment is indicated in pain which does not go, the progression of deformity and neurological deficits.
Selected patients get operated for cosmetic reasons also.
Postural thoracic kyphosis can often be treated with posture correction, education, and exercises.
Surgical Correction is indicated in patients and indications vary with the cause of the kyphosis.
- In Scheuermann kyphosis indications are
- Kyphosis greater than 75 degrees
- Kyphosis greater than 65° with pain
- Unacceptable appearance of the trunk
- balancing problems while sitting
- Skin problems at the apex of the deformity
- In kyphosis after trauma, surgery is considered
- Progressive neural deficit
- Kyphosis > 30 degrees
- > 50% loss of height
Significant cardiopulmonary risk and medical unfitness are contraindications for a surgical procedure.
Non-operative therapy for kyphosis consists of
- Exercise
- Medication
- NSAIDs
- Muscle relaxants
- Antibiotics in infection
- Bracing
- Effective in skeletally immature patients with Scheuermann disease
- Correction may get diminished as skeletal maturity occurs.
Physical therapy has not been proved effective.
Surgical correction of the deformity can be done via an anterior, a posterior, or a combined anterior-posterior approach.
The surgery carries the risk of following complications
- Neurologic deficit
- Manipulation, traction, or compression r
- Reduction of blood flow
- Pseudarthrosis
- Implant failure
- Prominent posterior hardware
- Wound infections
Results of surgical correction vary, depending on the cause of the deformity.
References
- Macagno AE, O’Brien MF. Thoracic and thoracolumbar kyphosis in adults. Spine (Phila Pa 1976). 2006 Sep 1. 31 (19 Suppl): S161-70.
- Malcolm BW, Bradford DS, Winter RB, Chou SN. Post-traumatic kyphosis. A review of forty-eight surgically treated patients. J Bone Joint Surg Am. 1981 Jul. 63 (6):891-9
- Murray PM, Weinstein SL, Spratt KF. The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am. 1993 Feb. 75 (2):236-48.
- Clement JL, Chau E, Kimkpe C, Vallade MJ.
- Ball JM, Cagle P, Johnson BE, Lucasey C, Lukert BP. Spinal extension exercises prevent natural progression of kyphosis. Osteoporos Int. 2009 Mar. 20 (3):481-9.