Last Updated on October 28, 2023
Calcaneus fracture or os calcis represent 2% of all fractures seen in adults. The os calcis is the most frequently fractured tarsal bone and accounts for more than 60% of tarsal fractures. Calcaneus is the bone that forms the heel. Calcaneus fractures are most commonly seen in young men.
Extra-articular fractures account for 30% of all calcaneus fractures in adults. The most common extra-articular fracture is a calcaneal body fracture.
10-15% of extra-articular injuries are represented by fractures of the anterior process of calcaneus The only type of calcaneus fractures that are more common in women].
Fractures of the superior tuberosity beak or avulsion fractures represent 10% of extra-articular injuries. sustentaculum tali fractures are rare.
Intra-articular fractures constitute 70% of all calcaneus fractures in adults.
Open injuries that have been reported to occur in 2-17% of cases.
Relevant Anatomy of Calcaneus



The calcaneus is the largest of the tarsal bones. It forms the heel of the foot and articulates with talus above and cuboid anteriorly.
Anteriorly the calcaneum articulates with cuboid.
The superior articular surface of calcaneus contains three facets that articulate with the talus. These are also called subtalar facets and function as a unit. Any interruption in their alignment constitutes an intra-articular fracture. These facets are
- Posterior facet is the largest and is the major weight-bearing surface [Flexor hallucis longus tendon runs just inferior to it]
- Middle facet is anteromedial on sustentaculum tali
- Anterior facet is often confluent with middle facet
Posterior facet is a major weight-bearing surface, though the anterior and middle facets bear more weight per unit area.
Sinus Tarsi [Calcaneus Part]
Between the middle and posterior facets lies the interosseous sulcus or calcaneal groove) that together with the talar sulcus makes up the sinus tarsi
Sustentaculum tali
- It is a medial projection of calcaneus and supports the neck of talus [Hence the name]
- Flexor hallucis longus passes beneath it
- It is connected by deltoid and talocalcaneal ligament to the talus
In calcaneal fractures, it is contained in the anteromedial fragment, which is one of the constant fragments in the calcaneal fracture. It is a constant fragment due to medial talocalcaneal and interosseous ligaments.
The sustentaculum tali is supported by the complex medial arch structures, including the insertion of the tibialis posterior tendon and the spring ligament. The fractures through the sustentaculum tali are a constant feature of all calcaneus fractures and, if not anatomically restored, will interfere with the medial arch.
A bifurcate ligament connects the dorsal aspect of the anterior process to the cuboid and navicular.
The body of the calcaneus has a comparatively thin cortex. But there are, however, several important areas of increased bony density that are particularly amenable to screw placement, including the following:
- Angle of Gissane [Explained in x-rays]
- Plantar posterior tubercle
- Anterior aspect of the anterior process
- Sustentaculum tali
The tibial artery, nerve, posterior tibial tendon, and flexor hallucis longus tendon course along the medial wall of the calcaneus
Laterally, the peroneal tubercle provides a groove for the peroneal tendons (the brevis superiorly and the longus inferiorly).
Calcaneus bone is subcutaneous, except on the heel pad. The soft tissue injury is, therefore, highly significant and may lead to many of the problems with surgical intervention
Internally, the os calcis contains compression and tensile trabeculae. The central portion of the middle third is fairly weak cancellous bone, especially weak in compression.
Causes of Calcaneus Fracture
Intraarticular fractures are often caused by traumatic axial loading is the primary mechanism of injury. It is often directed through the laterally situated (in relation to the weight-bearing axis) plantar tuberosity of the calcaneus.
Extra-articular injuries are more likely to occur with a sudden twisting force applied to the hindfoot than with other mechanisms
- Fall from height
- Motor vehicle collisions
- Impact on a hard surface while running or jumping
- Blunt-force injury [Causes extra-articular fracture of the calcaneus]
- Avulsion injuries with abrupt contraction of the Achilles tendon
- Overuse injury, or stress fracture
Pathophysiology
Intraarticular fractures
About 75% fractures are intraarticular.
Calcaneus fractures are typically caused by a high-energy axial load applied to the heel, which drives the talus downward onto the calcaneus.
Following axial loading, there may also be a rotational element, especially in varus. As the axial load is applied to the hindfoot, the talus is driven into the angle of Gissane, dividing the os calcis into two fragments.
This results in the primary fracture line extending from the lateral aspect of the angle of Gissane in a posteromedial direction, initiating an oblique, primary fracture line resulting in two primary fragments.
Superomedial fragment (constant fragment)
It includes the sustentaculum tali and is stabilized by strong ligamentous and capsular attachments. The constant medial fragment containing the sustentaculum tali remains in its anatomical position because of its strong soft tissues.
Superolateral fragment
It includes an intra-articular line through the posterior facet.
As the axial load continues, secondary fracture lines occur. These may involve the joint itself in a single or in multifragments, or the fracture line may be a single horizontal line resulting in a so-called tongue-type fracture described by Essex-Lopresti.
As the central portion of the posterior facet impacts into the underlining cancellous bone, the lateral wall is driven directly under the fibula, causing impingement to the soft tissues in that area.
There might be multiple secondary fracture lines may develop resulting in different patterns. Secondary fracture lines dictate whether there is joint depression or tongue-type fracture [See classification]
Extra-articular fractures
These fractures vary in causation according to areas of calcaneus affected
Strong contraction of gastrocnemius-soleus with concomitant avulsion at its insertion site on calcaneus would cause extrarticular fracture and is more common in osteopenic bone
Anterior process fractures may be caused by inversion and plantar flexion of the foot leading to avulsion of the bifurcate ligament.
Other Musculoskeletal Injuries Associated with Calcaneal Fracture
- Extension into the calcaneocuboid joint [63%]
- Vertebral injuries [10%]
- Contralateral calcaneus [10%]
Classification of Calcaneus Fractures
We have already discussed classification based on articular involvement. [Intra-articular and extra-articular]
Essex-Lopresti classification
Essex-Lopresti described two types of intra-articular fractures
The primary fracture line runs obliquely through the posterior facet forming two fragments. Essex Lopresti Classification is based on the orientation of secondary lines.
The secondary fracture line runs in one of two planes
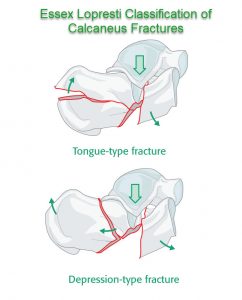
Tongue Type Fractures
It passes through the axial plane beneath the facet exiting posteriorly in tongue-type fractures. The superolateral fragment and posterior facet remain attached to the tuberosity posteriorly.
Joint depression fractures
The secondary line passes behind the posterior facet in joint depression fractures.
Sanders Classification
Type I
Nondisplaced posterior facet (regardless of the number of fracture lines)
Type II
One fracture line in the posterior facet (two fragments)
Type III
Two fracture lines in the posterior facet (three fragments)
Type IV
Comminuted with more than three fracture lines in the posterior facet (four or more fragments)
Clinical Presentation
There would be a history of trauma and severity of the trauma and presence of other injuries may affect the presentation.
Often there is a history of fall from the height or there would be a motor vehicle accident.
Patients are more likely to be young male individuals.
Other musculoskeletal injuries should be looked for too.
Compression fractures of the spine are common and should be particularly looked for.
Painful swelling is a common finding. There would be a presence of ecchymosis, deformity of the heel or plantar arch and Inability to bear weight on the injured foot.
Open injuries are surgical emergencies and should be dealt with accordingly.
Tenderness can be elicited by a gentle squeeze of the heel.
Ecchymosis that may tracks distally to the sole of the foot may be noted. This particular pattern of ecchymosis is known as the Mondor sign, is pathognomonic for calcaneal fracture.
The neurovascular examination should be conducted and compared to the opposite foot.
Paresthesia, edema, diminished pulses, or severe pain with passive flexion of the toes that might suggest compartment syndrome of the foot.
A complete musculoskeletal examination is indicated to rule out or establish any other injury.
Lab Studies
Lab workup is required as preoperative work. Complete blood count (CBC), blood typing, coagulation profile evaluation, and electrocardiography routine preoperative studies in calcaneus injuries. Additional studies, if warranted may vary from patient to patient.
Imaging
X-rays
AP, lateral, and oblique foot views are essential. Broden and Harris or axial views are optional.
AP View
Evaluation of
- Calcaneocuboid joint involvement
- Talonavicular subluxation
- Lateral wall widening
- Subfibular impingement [due to lateral displacement of the lateral wall of the calcaneus]
Lateral View
Apart from the visualization of fracture anatomy, evaluate the Bohler angle and angle of Gissane.

Bohler Angle
Also called Boehler angle, the angle is defined by two intersecting lines.
- One line is drawn from the anterior process of the calcaneus to the peak of the posterior articular surface
- Other line is drawn from the peak of the posterior articular surface to the peak of the posterior tuberosity.
The average Bohler angle is 25-40°. In severe fractures with subtalar joint involvement, this angle may decrease or become negative.
A normal Bohler angle though does not rule out a calcaneal fracture.
Angle of Gissane
Gissane angle is also known as the critical angle.
It is formed by the downward and upward slopes of the calcaneal superior surface.

Oblique view
It shows the degree of displacement of the primary fracture line and the lesser facets.
Broden View
Broden views of the foot are obtained by internally rotating the leg 45° with the ankle in a neutral position. The beam is directed toward the lateral malleolus and advanced cephalad at intervals of 10°, 20°, 30°, and 40° to fully evaluate the posterior facet.
It allows visualization of the posterior facet and is useful for evaluation of intraoperative reduction of the posterior facet
Harris view or Axial View
Axial views depict the primary fracture line, varus malposition, posterior facet stepoff, lateral-wall displacement, and fibular abutment.
It is taken by placing the foot in maximal dorsiflexion and angle the x-ray beam 45 degrees
Computed tomography
CT is considered the gold standard
- Axial views enable good visualization of the talonavicular and calcaneocuboid joints involvement, the anteroinferior aspect of the posterior facet, the sustentaculum tali, and the lateral calcaneal wall.
- Coronal views are oriented perpendicular to the posterior facet. [30-degree semicoronal] These views are important for distinguishing injury to the posterior facet.
- Sagittal view demonstrates tuberosity displacement
MRI
MRI is used to diagnose calcaneal stress fractures in the presence of normal radiographs. It is also used in uncertain diagnosis.
Treatment of Calcaneal Fractures
Extra-articular fractures are generally treated in a closed manner. Exceptions include
- fractures of the sustentaculum tali > 2 mm displacement
- Posterior avulsion fractures
- Significant fractures of the calcaneal body.
Intra-articular fractures are more commonly treated with a combination of
- Open reduction
- Ostectomy/ osteotomy
- internal fixation
- Arthrodesis of the subtalar and calcaneocuboid joints.
Treatment goals of operative modalities are the restoration of heel height and length, eealignment of the posterior facet of the subtalar joint and restoration of the mechanical axis of the hindfoot.
Depending on the injury, patient profile and comorbid conditions, different combinations may be attempted.
Surgery for calcaneus fractures should be delayed, ideally for 10-14 days, in the presence of significant edema or fracture blister formation except in open fractures and presence of compartment syndrome in the foot which is treated as emergency cases.
Nonoperative Treatment
Non-weight bearing Cast immobilization
It is done in calcaneal stress fractures and undisplaced intraarticular fractures and for extraarticular fractures.
In the initial period, the limb should be elevated, swelling kept to a minimum by icing or other techniques.
In stress fractures, the cast is applied for 6 weeks whereas in the other cases the cast is applied for 10 to 12 weeks. Throughout the period the cast is kept non-weight bearing. Ambulation can be allowed with support [crutches] and gradual restoration of full weight-bearing as pain disappears, usually at 8–12 weeks.
Indications for cast immobilization are
- Stress fracture
- Small extra-articular fracture (<1 cm)with intact Achilles tendon and <2 mm displacement
- Sanders Type I(nondisplaced)
- Anterior process fracture involving <25% of calcaneocuboid joint
- Comorbidities that preclude good surgical outcome
- Smoker
- Diabetes
- Peripheral vascular disease
Early range of motion exercises are begun once swelling allows.
Operative Treatment
Closed Reduction with Percutaneous Fixation
Indications
- minimally displaced tongue-type fractures
- Fractures with mild shortening
- Large extra-articular fractures (>1 cm)
Early reduction prevents skin sloughing and need for subsequent flap coverage.
The fixation can be done with screws or Steinmann pin.
Open Reduction and Internal Fixation
Indications
- Displaced tongue-type fractures
- Large extra-articular fractures (>1 cm) with
- The detachment of Achilles tendon and/or
- > 2 mm displacement
- Sanders Type II and III fractures
- Posterior facet displacement >2 to 3 mm
- Flattening of Bohler angle
- Varus malalignment of the tuberosity
- Anterior process fracture with >25% involvement of calcaneocuboid joint
- Displaced sustentaculum tali fractures
It is wise to wait for 0-14 days before operating to allow swelling and blisters resolve and wrinkle sign appear.
Primary subtalar arthrodesis
It is indicated in Sanders Type IV and is combined with open reduction and internal fixation to restore height
Open techniques may be performed by using medial, lateral, or combined approaches, depending on the extent of the injury and the location of the fracture fragments.
An extensile lateral L-shaped incision is most popular as it provides access to calcaneocuboid and subtalar joints but has a high rate of wound complications.
The medial approach can also be used. A full-thickness flap is created to maintain soft tissue integrity.
Open reduction and internal fixation of a calcaneus fracture are associated with a high incidence of postoperative wound infection and breakdown.
A suction drain is frequently used after open reduction and internal fixation and is removed when there is less than 10 mL of drainage over 8 hours.
Postoperatively, the foot is elevated for up to 72 hours to reduce postoperative swelling.
The range of motion exercises are begun usually 10-12 days after surgery. At this time A well-fitting orthosis is provided for comfort and to prevent gastrocnemius-soleus contracture. Sutures are removed at 2-3 weeks.
Weight-bearing is delayed up to 10-12 weeks.
Complications of Calcaneus Fracture
- Chronic disability and pain
- Subtalar or calcaneocuboid joint malfunction
- Subtalar arthritis
- Poor wound healing (10-25% of open injuries)
- Seen more in smokers, diabetics, and open injuries
- Lateral impingement with peroneal irritation
- Damaged FHL
- At-risk with the placement of lateral to medial screws
- Compartment syndrome (10%)
- Malunion
- Limited ankle dorsiflexion
- Infection
- Nonunion
Supervised physical therapy is beneficial, both during nonweight bearing and during the active weight-bearing.
Prognosis of Calcaneus Fracture
- Intra-articular fractures of the calcaneus result substantially higher morbidity
- The minimally invasive approach resulted in a lower postoperative complication rate
Factors associated with a poor outcome are
- Age > 50
- Obesity
- Manual labor
- Smokers
- Bilateral calcaneal fractures
- Multiple trauma
- Vasculopathies
References
- Browner B, Jupiter J, Levine A. Skeletal Trauma. 2003. 1:2406-34.
- Sanders R. Fractures and fracture-dislocations of the calcaneus. Surgery of the Foot and Ankle. 1999. 2:1422-1464.
- Juliano P, Nguyen HV. Fractures of the calcaneus. Orthop Clin North Am. 2001 Jan. 32(1):35-51, viii.
- Buckley R, Tough S, McCormack R. Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am. 2002 Oct. 84-A(10):1733-44.
- Benirschke SK, Sangeorzan BJ. Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures. Clin Orthop. 1993 Jul. 128-34
- Potter MQ, Nunley JA. Long-term functional outcomes after operative treatment for intra-articular fractures of the calcaneus. J Bone Joint Surg Am. 2009 Aug. 91(8):1854-60.