Last Updated on October 27, 2023
Calcaneus is bone of the hindfoot and is the largest tarsal bone. Calcaneus forms the prominence of the heel.
Structure of Calcaneus
Calcaneus is roughly cuboidal in shape. It is directed forwards, upwards and laterally.
It has six surfaces.
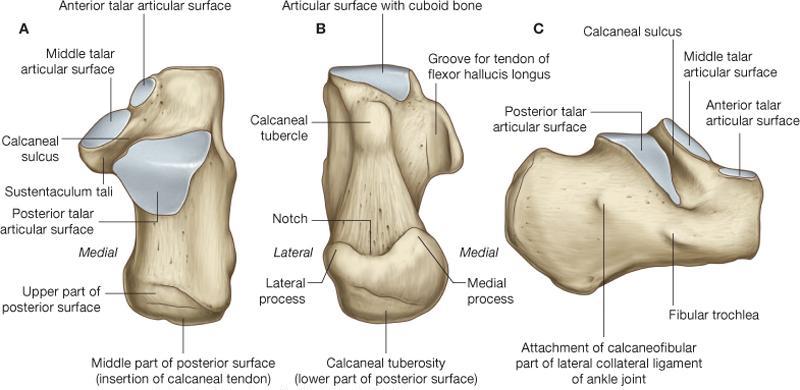
Anterior Surface
The anterior surface is the smallest surface of the bone. It is covered by a concavoconvex, sloping articular surface to the calcaneocuboid joint and is roughly triangular. It is concave in an oblique inferolateral plane and convex in a plane perpendicular to this.
Posterior Surface
The posterior calcaneal surface is convex, dome-shaped, wider inferiorly, and has 3 distinct areas – upper, middle and lower.
The upper area is smooth, slopes anteriorly, and supports a bursa, which lies between it and the Achilles tendon.
The middle part gives insertion to the Achilles tendon
The lower part is covered by fibrofatty tissue of the plantar heel pad
Superior Surface
The superior calcaneal surface of the calcaneus has 2 parts: articular and nonarticular.
The nonarticular part has variable length and extends posteriorly to form the heel. It is about one-third of total superior surface.
It is convex from side to side, is concave in the anteroposterior axis, and supports a fat pad situated anterior to the Achilles tendon.
Anterior to this nonarticular part is articular which has an oval facet facing superiorly and is tilted anteriorly. The articular portion of the superior surface is convex in the anteroposterior axis and articulates with the posterior calcaneal facet on the undersurface of the talus.
Calcaneus sulcus is deep groove anterior to posterior facet and directed posteromedially It matches the inferior similar sulcus on the lower surface of the talus, and both these grooves form a canal in the hindfoot called the sinus tarsi.
Anteromedial to the calcaneal sulcus is an articular area, elongated and concave in its long axis and directed anterolaterally. A transverse notch divides this into larger middle facet posteriorly and anterior facet.
The middle facet lies on a medially projecting process of the calcaneus called the sustentaculum tali. It articulates with the middle calcaneal facet on the undersurface of the talus.
The anterior facet lies on the anterior process of the calcaneus and articulates with the anterior calcaneal facet on the talus.
The upper rough surface, anterior and lateral to the facets, is rough for the attachment of ligaments and for the origin of the extensor digitorum brevis.
Plantar surface
The inferior or plantar surface is wider posteriorly and convex from side to side.
It has a prominence at the back, called the calcaneal tuberosity. Calcaneal tuberosity has a central longitudinal depression dividing it into a smaller lateral and larger broader medial process.
The lateral process gives rise to part of the abductor digiti minimi whereas the medial process that gives attachment to the abductor hallucis, front to the flexor digitorum brevis and the plantar aponeurosis.
Lateral Surface
The lateral surface is rough and almost flat, broader posteriorly and narrowed anteriorly. Anteriorly, a small elevation termed the peroneal fibular] tubercle or trochlea is present.
It is a ridge that separates two grooves. The superior groove is for peroneus brevis tendon and inferior is for peroneus longus tendon.
Av small tubercle in the middle of the lateral surface gives attachment to, to which the calcaneofibular ligament.
Medial surface
The medial surface is concave from above downwards. The concavity is accentuated by the presence of a medially oriented shelf-like projection of bone, called the sustentaculum tali, which projects medially from its anterosuperior border. The sustentaculum tali have an articular surface for the middle calcaneal facet and is grooved inferiorly to house the flexor hallucis longus tendon Its lower surface is grooved, and the medial margin is in the form of a rough strip convex from before backward.
Attachments and relations of the calcaneus
Attachments on Posterior Surface
The middle rough area on the posterior surface receives the insertion of the tendocalcaneus and of the plantaris. The upper region is covered by a bursa. The lower area is covered by dense fibrofatty tissue and supports the body weight while standing.
Attachments on Dorsal or Superior Surface
The lateral part of the nonarticular area on the anterior part of the dorsal surface provides;
- Origin to the extensor digitorum brevis
- Attachment to the stem of the inferior extensor retinaculum
- Attachment to the stem of the bifurcate ligament
Sulcus calcanei provides attachment to the interosseous talocalcaneal ligament medially, and the cervical ligament laterally.
Attachments on Plantar Surface
The attachments on the plantar surface are as follows;
The medial tubercle
- Medially
- The origin for the abductor hallucis
- Attachment to the flexor retinaculum
- Anteriorly
- Flexor digitorum brevis
- Attachment to the plantar aponeurosis
The lateral tubercle
- Origin to the abductor digiti minimi, the origin extending to the front of the tubercle.
- The anterior tubercle
- Along with the rough area in front – short plantar ligament.
- The rough strip between the three tubercles – Long plantar ligament.
Attachments on Lateral Surface
The peroneal tubercle – Slip from the inferior peroneal retinaculum.
The calcaneofibular ligament is attached about I cm behind the peroneal trochlea.
Attachments on Medial Surface
- The groove on the lower surface of the sustentaculum tali is occupied by the tendon of the flexor hallucis longus.
- The medial margin of the sustentaculum tali
- Spring ligament
- Slip from the tibialis posterior in the middle
- Superficial fibers of the deltoid ligament along the length
- Medial talocalcaneal ligament posteriorly.
- Below the groove for the flexor hallucis longus, the medial surface gives origin to the fleshy fibers of the medial head of the accessory flexor digitorum.
Ossification
- One primary and one secondary center.
- Primary center – During the 3rd month of intrauterine life.
- Secondary center 6-8 years to form a scale-like epiphysis on the posterior surface
- Fuses with the rest of the bone by 14-16 years.
Side Determination of Calcaneus
- The anterior surface is small and bears a concavoconvex articular facet for the cuboid.
- The posterior surface is large and rough.
- The dorsal or superior has a large convex articular surface in the middle.
- The plantar surface is large and triangular.
- The lateral surface is flat
- The medial surface concave from above downwards.
Blood Supply of Calcaneus
Blood supply of calcaneus is by calcaneal branches which arise from deep perforator peroneal and posterior tibial arteries.
Clinical Significance of Calcaneum
- Gastrocnemius, soleus, and plantaris are posterior compartment muscles of the leg and aid in walking, running and jumping. Their specific functions include plantarflexion of the foot, flexion of the knee, and steadying the leg on the ankle during standing.
- Calcaneal is frequently injured bone, especially in fall from height. Most of the calcaneal fractures are treated by nonoperative means but surgery for displaced fractures is required.
- Calcaneal is surrounded by minimal soft tissue and surgical incisions need to be carefully planned because of wound healing problems in the area.