Last Updated on October 28, 2023
Scoiliotic curves can be classified by many approaches. We are describing two mainly used methods for classification of scoliosis curves.
These classifications are named as Ponseti and Friedman, and Kings’s classification of scoliosis curves.
Scoliosis, as we know, is of non-idiopathic and idiopathic types. Neuromuscular and degenerative scoliosis are types of non-idiopathic scoliosis.
Ponseti and Friedman Classification of Scoliosis Curves
It is a simple classification based on where the curve is located.
Single major lumbar curve.
The lumbar curve has its apex between the L1-2 disc and L4 producing an asymmetry of the waistline with prominence of the contralateral hip.
Single major thoracolumbar curve.
The thoracolumbar curve apex is at T12 or L1 and tends to produce more trunk imbalance than other curves. It often produces a severe cosmetic deformity.
Combined thoracic and lumbar curves (double major curves).
Causes less visible deformities because the trunk usually is well balanced.
Single major thoracic curve.
Generally is a convex right pattern. The curve produces prominence of the ribs on the convex side, depression of the ribs on the concave side, and elevation of one shoulder.
Single major high thoracic curve.
The apex of the curve usually is at T3, and the curve extending from C7 or T1 to T4 or T5.
Double major thoracic curve.
There is a short upper thoracic curve, often extending from T1 to T5 or T6, with a considerable rotation of the vertebrae and other structural changes and a lower thoracic curve extending from T6 to T12 or L1.
The upper curve usually is convex to the left, and the lower usually is convex to the right.
King Classification
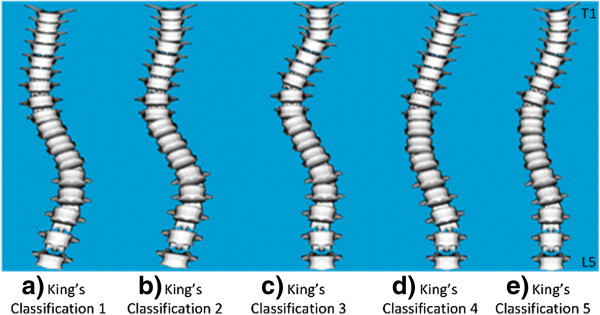
This classification system of scoliosis curves is used to describe thoracic curves.
Type I curve
The lumbar curve is larger than the thoracic curve or nearly equal, but the lumbar curve is less flexible on side bending.
Type II curves
A combined thoracic and lumbar curve and the thoracic curve is larger than or equal to the lumbar. On supine side-bending radiographs, the lumbar curve is more flexible than the thoracic curve.
Type III curve
Thoracic scoliosis with the lumbar curve not crossing the midline.
Type IV curve
Single long thoracic curve, with L4 tilted into the curve and L5 balanced over the pelvis.
Type V curve
A double structural thoracic curve. The first thoracic vertebra is tilted into the concavity of the upper curve, which is structural. An elevation of the left shoulder is a frequent finding. There is an upper left thoracic rib hump and a lower right thoracic rib prominence.
Ponseti-Friedman Classification
- Type I
- Single major lumbar curve at T11-L3
- Apex at L1-2
- The most benign curve
- Affects 23% of patients.
- Type II
- Single major dorsolumbar curve at T6-7 to L1-2
- Apex at T11-12
- Found in 16%
- Type III
- Combined thoracic and lumbar
- Dorsal curve on the right side at T5-6 or T10-11,apex at T7-8
- Lumbar curve on the left side at T10-11 to L3-4, apex at L1-2.
- Type IV
- Single major thoracic curve at T5-6 to T11-12
- Apex at T8-9
- Type V
- Cervicothoracic at C7-T1 or T4-5 with
- Apex at T3.
Lenke’s Classification
Lenke’s classification system is used for Adolescent idiopathic scoliosis. It is a triad of classification system which takes into following
- Curve type [1-6]- there are six types of the curve defined on various parameters and measurements
- Lumbar spine modifier (A, B, C) – Lumbar spine modifier is determined by marking a vertical line from the center of sacrum Nd where it touches the apical vertebra.
- Sagittal thoracic modifier (-, N, +)- it is determined from the he lateral radiograph from T5-T12 and measure presence of kyphosis and designated as (-),N or (+) A
Because Lenke’s classification is quite exhaustive in itself, it has been discussed separately.