Last Updated on October 28, 2023
Axillary nerve injury can result either from compression of the axillary nerve or traumatic injury resulting from traction, direct trauma or from injections.
As deltoid is the muscle that is being supplied along with skin over the deltoid area, the axillary nerve injury causes deltoid muscle paralysis and numbness over the region.
Axillary nerve injury is reported to be 0.3% to 6% of the brachial plexus injuries.
The clinical presentation of axillary nerve dysfunction is variable. It can be missed due to the presence of concomitant injuries like dislocation or fracture. and can go undetected, as the concomitant dislocation or fracture may mask the symptoms. Nerve injury should be considered as part of the differential diagnosis process when a patient reports pain, weakness, or paresthesias.
Anatomy of Axillary Nerve
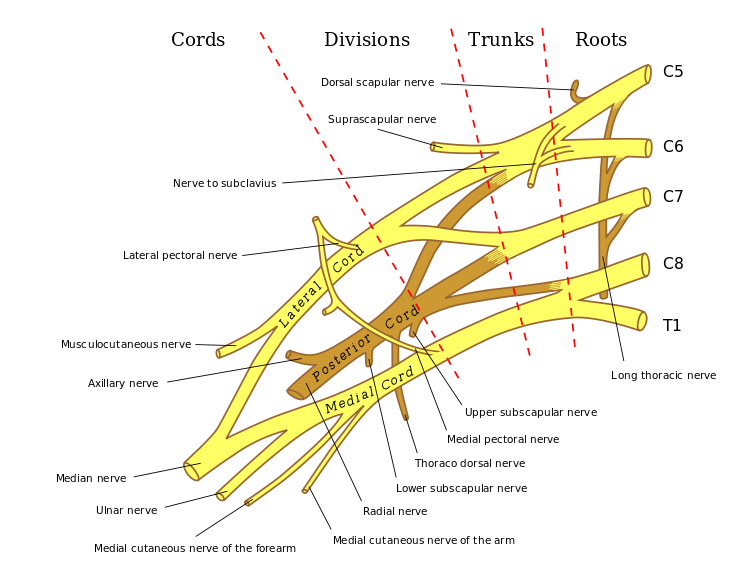
Axillary nerve originates from the posterior cord of brachial plexus and carried C5 and C6 fibers.
After its formation, it lies to anterior to the subscapularis muscle and posterior to the axillary artery.
It courses along anterior subscapularis to inferior end and then exits the axilla posteriorly via the quadrangular space. It is accompanied by the posterior circumflex humeral artery.
Quadrangular space is in the posterior scapular region, which is bounded by the superior margin of the teres major inferiorly, the inferior margin of the teres minor superiorly, the lateral margin of the long head of the triceps brachii medially and the surgical neck of the humerus laterally.
Here, the axillary nerve supplies a branch to the shoulder joint [articular branch] The posterior circumflex humeral artery and vein also run posterior to this nerve in this space.
The nerve divides into anterior and posterior terminal branches within the quadrangular space. The anterior
The anterior branch wraps around the surgical neck of the humerus, running in the deep deltoid fascia with the posterior circumflex humeral artery. Anterior branch has been shown to run 5-7 cm distal to the lateral edge of the acromion
It supplies the anterior deltoid muscle and terminates in small cutaneous branches supplying the anterior and anterolateral shoulder.

Posterior branch supplies the teres minor and posterior deltoid muscles. It is the most susceptible to injury during arthroscopy. It terminates at the superior lateral brachial cutaneous nerve supplying the lateral shoulder.
Causes of Axillary Nerve Injury
Causes of Axillary Nerve Injury
- Anterior shoulder dislocation
- Blunt trauma
- Injection palsy
- Injury during arthroscopy
- Quadrangular space syndrome Compression of the axillary nerve within the quadrangular space in overhead athletes Muscle hypertrophy or paralabral cysts are the causes
Clinical Presentation
The usual presentation is not acute often masked by other injuries. A motor and sensory examination in the acute situation are not certain too as the presence of pain/deformity would affect movements and ability to judge sensory examination input.
The patient presents a duration after the injury, often when another injury has been taken care of, generally after 2-4 weeks.
There are complaints of generalized mild, dull, and ache which is deep or on the lateral shoulder. Occasionally, the pain could radiate to the proximal arm.
There would complain of numbness and paraesthesiae of the lateral arm and/or posterior aspect of the shoulder
There may be a feeling of the shoulder of instability and shoulder weakness.
Weakness is especially pronounced in flexion, abduction, and external rotation.
Not all persons are symptomatic though.
Some athletes may complain of weakness and early-onset fatigue with exercise only, especially with overhead activities and heavy lifting.
History of trauma may always be not available.
Though rare intramuscular injections in deltoid may injure the nerve and should be probed in absence of clear trauma.
On examination, there would be an area of hypoaesthesia on the lateral aspect of the upper arm, typically in the region where regimental badges used to be placed. Typically, the lower half of the deltoid.
Motor supply of axillary nerve is to teres minor and deltoid and depending on the level of injury there would be the weakness in both these muscles or only in the deltoid.
There would be visible muscle atrophy of the deltoid and teres minor.
A complete examination of the shoulder should be done.
The findings would vary with the extent of damage to the axillary nerve.
Clinical Tests
Lag sign test
The physician stands behind the patient and elevates the patient’s arm.
The patient is asked to hold this position without the doctor’s assistance. If the patient cannot hold this position on their own and an angular drop occurs, it indicates deltoid weakness.
Hornblower’s test
This test detects teres minor weakness. For this test place shoulder in 90° abduction and 90° external rotation. The test is considered positive if patient unable to maintain external rotation, arm falls into internal rotation
Investigations
Electromyography is the diagnostic test of choice to identify nerve conduction loss but the changes may not be identifiable until 2-3 weeks after injury. Electromyography is also able to distinguish between atrophy secondary to pain or nerve injury.
It can also be used to monitor the progression of the injury.
Treatment of Axillary Nerve Injury
The choice of treatment is determined by the type of injury
The prognosis worsens with the severity of the injury.
Conservative Treatment
Patients with grade I and II [neuropraxia and most of the patients with neuropraxia [grade 1 injury] recover with conservative management within 6 to 12 months.
Patients with axonotmesis (2nd degree) nerve injury, the recovery rate is about 80%.
The patient should be put on conservative treatment and if there are no signs of functional return by 6 months, surgical exploration and possible nerve grafting are recommended.
Patients with neurotmesis (nerve transection) there is typically no recovery without surgical intervention.
Moreover, the prognosis is better if the surgery is performed within 6 months of the injury.
In acute closed injuries with axillary nerve injury, the treatment of the injury takes precedence.
In closed injuries, an immediate reduction would cause the nerve to relax and has better chances of responding to conservative treatment.
In open injuries, the exploration may be indicated depending on the severity of the wound.
Conservative treatment for nerve injury consists of maintaining joint range of motion while waiting for nerve recovery.
For local symptoms like pain, relevant drugs may be taken.
Surgical Treatment
Surgical treatment is considered at the outset for axonotmesis [complete transection].
It can be done immediately where a compression or injury is due to a structure that needs removal. For example, an osteophyte I quadrilateral space.
Indications for Surgery
- Compression in the quadrilateral space
- No clinical or EMG improvements seen after 3 to 6 months of injury/conservative treatment.
Choice of surgical procedures available
- Neurolysis – When the nerve is intact but compressed by surrounding tissue
- Nerve repair
- Nerve grafting – To fill the gap between the nerve ends
- Nerve transfer – Usually using triceps motor branch
After surgery, the shoulder should be immobilized for 4 to 6 weeks and followed by rehabilitation.