Last Updated on October 15, 2023
Intradiscal electrothermal therapy (IDET) or intradiscal electrothermal annuloplasty (IDEA) consists of the percutaneous threading of a flexible thermal catheter into the disc under fluoroscopy to heat the posterior annulus of the disc thereby leading to the contraction of collagen fibers and destruction of pain receptors.
Intradiscal electrothermal therapy is a minimally invasive form of annuloplasty. Annuloplasty means the repair of annulus fibrosus.
It is a relatively new procedure and initial studies have shown encouraging results. Sall and colleagues introduced this procedure in 1977 for discogenic back pain.
Relevant Anatomy
The intervertebral disc is a fibrocartilage structure that sits between two vertebral bodies in the cervical, thoracic, and lumbar spine. It consists of two components
- Outer annulus fibrosus
- Inner soft nucleus pulposus
The discs act as shock absorbers and thus provide cushion during the loading of the spine.
The disc may fail due to excessive loading acutely or repetitive injury. The failure of the disc is associated with
- Inflammation
- Dehydration of the nucleus
- Tear pf annulus
Annulus fibrosus contains pain receptors that are stimulated by tears extending to the periphery of the annulus.
This might result in discogenic pain that presents as back pain which may be associated with radiculopathy.

How Does Intradiscal Electrothermal Therapy Work?
Intradiscal electrothermal therapy is thought to decrease discogenic pain by thermal modification of collagen fibers and destruction of disc pain receptors but the exact mechanism of action is not clear yet. The proposed mechanisms are
- Collagen modification leads to alteration of spinal mechanics
- Stimulation of outer annulus fibrosus to heal
- Healing of annular fissures
- Decreased intradiscal pressure
- Cauterization of vascular ingrowth
None of these mechanisms have been proven yet.
Indications of Intradiscal Electrothermal Therapy
Intradiscal electrothermal annuloplasty should be considered in patients who have had discogenic low back pain for more than 6 months and whose condition has not responded to conservative treatment.
IDET is indicated for
- Persistent low back pain for 3-6 months with failed response to conservative measure
- No/ minimal radicular pain and normal neurologic exam
- MRI findings
- No neural compression or impairment
- Annular tears.
- Disc protrusions of size less than 3 to 4 mm.
- At least 50% remaining disc height
- Single-level disc affected
Ideally, the procedure should be considered in people less than 55 years of age and nonsmokers.
Contraindications
- Severe disc degeneration (Loss of more than half disc height)
- A disc that has extruded or sequestered
- Prominent radiculopathy
- Stenosis
- Spinal instability
- Failed intradiscal discal electrothermal therapy
Preferably not considered for patients older than 55 years because they are likely to have poor healing response. For a similar reason, the procedure is not selected for people who smoke.
Procedure
Assessments should be done to rule out the possibility of a nerve root compromise or impairment. Ideally, discography should be done to confirm the disc responsible for pain but the procedure itself is painful and done in select patients only.
The disc is approached in a similar manner to discography.
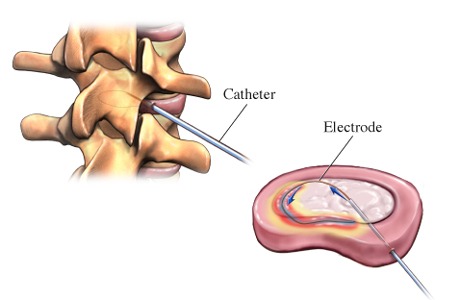
- A 17G introducer needle is inserted into the disc, under fluoroscopy.
- The position of the needle in the nuclear cavity is established by anteroposterior and lateral fluoroscopic views
- The thermal catheter is inserted through the needle.
- Once positioned the catheter is heated from 37°C to 65 °C.
- Temperature is kept at 65° for 1 minute
- Increase temperature by 1°C every 30 seconds until it is between 80° and 90°C.
The actual temperature of the annular tissue is as much as 15°C lower than the temperature of the catheter tip.
The patient may feel mild pain during this time. Each heating cycle takes about 20 minutes. More than one heating cycle per disc may be required.
After the procedure patient is shifted to the recovery room.
After Care
Recovery is not immediate but gradual. In fact, some patients may have increased pain for the initial few days. Significant pain relief may take 2-3 months.
The return to activity should be gradual. Physical therapy is an integral part of aftercare.
The patient should avoid lifting, bending, and prolonged sitting. Return to vigorous sports or athletic activity may take as much as 6 months.
Complications
IDET is associated with a very low rate of complications. The reported complications are
- Accelerated disc degeneration
- Spondylodiscitis
- After procedure headache
- Vertebral osteonecrosis
- Nerve root injuries were reported
- Catheter breakage
- Superficial skin burn
Effectiveness of Intradiscal Electrothermal Therapy
Some authors have reported reported improvement in symptoms following IDET. It appears to be effective in 60-70% of patients with chronic discogenic low back pain. However, there is a debate regarding its effectiveness as the evidence lacks consistency.
Further studies are needed for validation but the procedure appears promising.
References
- Derby R, Baker RM, Lee CH, Anderson PA. Evidence-informed management of chronic low back pain with intradiscal electrothermal therapy. Spine J. 2008;8:80–95. [link]
- Freeman BJ. IDET: a critical appraisal of the evidence. Eur Spine J. 2006;15:S 448–57.
- Helm Ii S, Simopoulos TT, Stojanovic M, Abdi S, El Terany MA. Effectiveness of Thermal Annular Procedures in Treating Discogenic Low Back Pain. Pain Physician. 2017 Sep;20(6):447-470.
- Kloth DS, Fenton DS, Andersson GB, Block JE. Intradiscal electrothermal therapy (IDET) for the treatment of discogenic low back pain: patient selection and indications for use. Pain Physician. 2008 Sep-Oct;11(5):659-68.
- Freeman BJ, Fraser RD, Cain CM, Hall DJ, Chapple DC. A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine(Phila Pa 1976). 2005 Nov 01;30(21):2369-77.