Last Updated on November 19, 2019
True and apparent leg length refer to limb lengths in absolute terms and in compensated forms. The limb length measurement is used to find leg length discrepancy if any.
When there is a shortening of the limb, the body compensates by tilting the pelvis down, equinus position of the foot and flexion of the opposite lower limb at the hip and knee.
True and Apparent Leg Length
True length is the measurement taken from the anterior superior iliac spine to the tip of medial malleolus while both lower limbs are in identical positions and the pelvis is square. Please note that identical position of the lower limb is and pelvis squaring is very important because the upper reference point ASIS [anterior superior iliac spine] is outside the limb and any change in the position can affect the length.
Actual true limb length should be measured from mid of head of the femur to medial malleolus but lack of reference point makes us select anterosuperior iliac spine, an easy to locate reference point.
Apparent length is measured in a similar way with the following differences
- The pelvis is not squared
- The limbs are not brought into the identical position
- The upper reference point is common [xiphisternum, umbilicus]
In nutshell, the deformity is left as such and limb length is measured from a common point such as xiphisternum or umbilicus.
For finding the apparent and true shortening, both the limbs are measured separately and the difference of the measurements is calculated. Apparent shortening means the difference between apparent leg lengths of two limbs.
True shortening means the difference between two true lengths.
Apparent shortening signifies the effect of deformity on the true shortening.
- If the true shortening is equal to apparent shortening it indicates there is no compensation.
- If the true shortening is more than the apparent one it indicates that part of the shortening has been compensated for
- If the true shortening is less than the apparent shortening it suggests a fixed adduction deformity in addition to shortening without any compensation
The shortening has a better term for it – leg length discrepancy but for the article, we would continue with the term.
How to Examine Leg Shortening?
Block Method
It uses the block adjustment method in the standing weight-bearing position. Usually, the patient compensates for shortening by abducting the leg. Correct the deformity first while keeping the trunk erect.
Correction of the deformity is suggested by iliac spines being at the same level.
As soon as both ASIS are level insert wooden blocks beneath the affected foot so as to keep up that level. The height of the wooden block required is the limb length disparity.

Supine Position
The pelvis is should be square to the table. The legs should be put in equivalent positions if possible.
In case of few deformities like pelvic tilting due to an adduction contraction of the hip, it will not be possible to do this.

In such cases, the pelvis is squared up and the limb length from ASIS to the tip of the medial malleolus is measured in the deformed position of the limb.
Now when the opposite limb is being measured for comparison it is necessary that it be placed in the position as that of the affected limb.
For better results, the landmarks should be marked before the measurement.
How to Keep Limb Position in Different Deformities for Leg Length Measurement
Abduction/Adduction Contracture of the Hip
When hip gets fixed in abduction, the pelvis is dipped towards the affected side to align the leg. This makes the normal leg appears shortened and the affected leg lengthened.
The opposite occurs with an adduction deformity.T
How to check for deformity?
- If both anterosuperior iliac spines or ASIS are at the same level and the pelvis is square there is no adduction or abduction deformity
- If the ASIS on the affected side is higher, a fixed adduction deformity is present.
- If the ASIS on the affected side is lower, a fixed abduction deformity is present.
Now, if there is a fixed deformity, either adduction or abduction, you cannot square the pelvis by moving the affected limb. Therefore the rule is to obtain an accurate comparison of their true length by surface measurement the two limbs must be placed in comparable positions relative to the pelvis.
[This only becomes necessary as our upper reference point is external. If we could measure somehow from the head of the femur, we would not need the squaring. Following diagram would explain this.
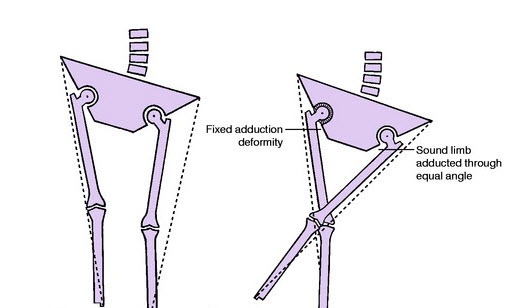
Thus if one limb is adducted and cannot be brought out to the neutral position, the other limb must be adducted through a corresponding angle by crossing it over the first limb before the measurements are taken.
This maneuver makes both limbs in comparable positions and the values arrived at would remove any fallacy.
Therefore, in adduction deformity – adduct the other limb through the same degree
and in abduction deformity – abduct the other limb through the same degree
Where is the Shortening?
After shortening has been found in the affected limb, the next question to be answered is the location of shortening.
Is it femoral or tibial?
Femoral or tibia origin can be determined by measuring thigh lengths and lower leg lengths individually and compared to the opposite side.
Galleazzi’s test
It is a gross test to find out if the shortening is in the femur or tibia.
The patient is supine with the hips flexed to 45º and the knees flexed up to 90º. Place the malleoli together(the test is inaccurate if you are unable to do so). Assess the position of the knees.
- When one knee projects farther forwards – the problem lies with the femur
- When one knee is higher than the other – tibia is the culprit
Where in Femur?
Tibial discrepancies are fairly straightforward to investigate.
However, same is not true for femur because of its deep-seated anatomy in the hip region.
The question that one needs to ask in femoral shortening is whether the shortening is supratrochanteric or infratrochanteric.
As the name suggests, the reason for supratrochanteric shortening lies above the trochanter and for infratrochanteric, it is below trochanter.
Shortening above the trochanter may be caused by the destruction of the femoral head or acetabulum or both, a dislocated hip, coxa-vara deformity of a malunited intertrochanteric fracture.
Various tests and measurements can help to answer these questions.
Bryant’s triangle

Bryants triangle test involves officially drawing out with pen various lines on the pelvis
- A perpendicular line is dropped from the anterior superior iliac spine onto the bed.
- From the tip of the greater trochanter, another perpendicular line is dropped onto the first line. it forms the base of the triangle.
- The length of the base [between the greater trochanter and ASIS ] is measured. Relative shortening on one side indicates that the femur is displaced upwards as a result of a problem in or near the hip joint.
Bryant triangle is not helpful in bilateral pathologies..
Nelatons line

Nelaton’s line connects the anterior superior iliac spine and ischial tuberosity. In cases of supra-trochanteric shortening, the trochanter will be proximal to this line.
Schoemaker’s line

- Patient lies supine
- A line joining the anterior superior iliac spine and tip of the greater trochanter is extended on the side of the abdomen on both sides.
- Normally, these lines meet in the midline above the umbilicus.
- Proximal migration of greater trochanter the lines will meet on the opposite side of the abdomen and below the umbilicus.
- If the problem is bilateral the lines will meet at or near the midline but below the umbilicus.
Chiene’s line or parallelogram
- Patient lies supine.
- Join both anterosuperior iliac spines.
- Join both trochanters.
- Normally the two lines are parallel. The lines would converge on the side of the proximal migration of trochanter, indicating supratrochanteric shortening.