Last Updated on November 10, 2019
The elbow joint is made up of three bones, the humerus, ulna, and radius.
Elbow joint connects the proper arm to the forearm. It is a synovial joint structurally but functionally is a hinge joint.
Elbow joint allows flexion and extension.
There are actually three joints at the elbow.
- Humeroulnar joint – Hinge joint formed between the humerus and the ulna. Allows flexion and extension of the elbow
- Humeroradial joint– Between the radius and humerus. Participates in flexion and extension but more importantly in supination and pronation of the forearm.
- Proximal radioulnar joint – A pivot joint formed by the radius and ulna. It participates in supination and pronation as well.
 In anatomic position [elbow is extended, the forearm is supinated], the long axis of the forearm has a lateral inclination or valgus at the elbow. This is called carrying angle and is measured to be 13± 5 degrees for females and 11 ± 4 for females.
In anatomic position [elbow is extended, the forearm is supinated], the long axis of the forearm has a lateral inclination or valgus at the elbow. This is called carrying angle and is measured to be 13± 5 degrees for females and 11 ± 4 for females.
Read the following articles for details of bones participating in elbow joint.
Bones of Elbow Joint
The elbow joint is composed of the distal end of the humerus and the proximal ends of the radius and the ulna.
Distal End of Humerus
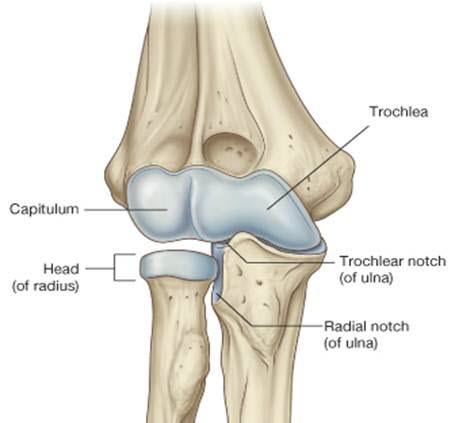
Humeral condyle, the distal end of the humerus is made up of the capitellum laterally and the trochlea medially. This condyle is covered by articular cartilage and articulates with trochlear notch of the ulna and the concave superior aspect of the head of the radius.
The axis of trochlea is externally rotated by 3 -8 degrees and compared with the longitudinal axis is in 4- 8° of valgus. The articular surface of the trochlea and capitellum is projected anteriorly at an angle of 40° to the axis of the humerus.
The trochlea, the distal medial articulating end of the humerus acts as a pulley for the ulnar trochlear notch to rotate around as the elbow is flexed.
The capitellum is a rounded ball of bone adjoining that adjoins trochlea laterally. It is the distal lateral articulating end of the humerus. It articulates with the radial head.
Superior to the articulating surface, the middle of the width of the humerus is marked by two depressions. On the anterior surface, it is coronoid fossa that accommodates the coronoid process of the ulna on flexion. Lateral to it is a smaller fossa called radial fossa that accepts radial head on flexion.
A depression on the posterior aspect is called olecranon fossa which accommodates the olecranon of the ulna on the extension. The olecranon is the proximal end of the ulna, from which the C-shaped trochlea notch is carved.
Lateral to the humeral condyle are the medial and lateral epicondyles, and superior to those on their respective sides are the medial and lateral supracondylar ridges.
The epicondyles and ridges serve as attachment sites for ligaments and muscles. Medial epicondyle serves as the origin of flexor muscles of forearm and hand whereas lateral epicondyle serves as extensor origin.
Ulna
The upper end of ulna provides articular cartilage–covered trochlear notch carved out of the olecranon process. The olecranon posteriorly serves as attachment of triceps muscle, a powerful elbow extensor.
Anteriorly, the trochlear notch ends in a blunt central point called the coronoid process.
The tuberosity of the ulna lies inferior to the coronoid process on the anterior aspect of the ulna. After that, further distally, is the shaft.
Laterally the coronoid process is the radial notch, in which lies the head of the radius.
Radius
Head of the radius bone is the main participant in the elbow joint. Its superior aspect contributes to the hinge portion of the elbow joint. The medial circumferential aspect of the head of the radius forms the radioulnar articulation.
After the head, the bone narrows distally into the neck. Anteromedially, a thick structure is called Distal to the head of the radius is a narrowing of the bone, referred to as the neck, and anteromedially is the radial tuberosity, followed distally by the shaft.
Joint capsule and Ligaments
The joint capsule is contiguous between the hinge and radioulnar aspects of the joint. The capsule has an outer fibrous layer and inner synovial layer.
The superior aspect of the joint capsule begins just superior to the coronoid and olecranon fossae and continues inferiorly, covering just past the proximal radial-ulnar articulation.
The ulnar collateral ligament is medial thickened part of the capsule.
Ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid and olecranon of the ulna. It is a triangular thickening with 3 main bands
- Anterior or cordlike band
- A posterior fan like band
- Oblique band
- The oblique band also helps to deepen the trochlear notch.
The radial collateral ligament is the lateral thickening and extends from the lateral humeral epicondyle and distally blends into the annular ligament of the radius.
The annular ligament of the radius wraps around the head of the radius and attaches to the ulna anteriorly and posteriorly. It allows the head of the radius to rotate inward during supination and pronation while maintaining the stability of the radial ulnar joint.
Muscles of the Elbow Joint
The biceps brachii, brachialis, brachioradialis, and pronator teres all flex the elbow and lie anteriorly. The triceps brachii and anconeus serve to extend the elbow and lie posteriorly.
The supinator and biceps brachii function to supinate the forearm at the elbow and the pronator teres and pronator quadratus pronate the forearm.
Movements are caused as follows
Extension: Triceps brachii and anconeus
Flexion: Brachialis, biceps brachii, brachioradialis
Bursae of Elbow Joint
- Intratendinous – located within the tendon of the triceps brachii.
- Subtendinous – between the olecranon and the tendon of the triceps brachii.
- Subcutaneous – between the olecranon and the overlying connective tissue.
Nerve supply of Elbow Joint
The elbow joint is supplied by the musculocutaneous, radial, and ulnar nerves.
Nervewise, the inferior lateral cutaneous nerve of the arm and the posterior cutaneous nerve of the forearm supply lateral elbow. The medial cutaneous nerve of the forearm supplies sensation to the medial aspect of the elbow. The cubital fossa is supplied by musculocutaneous nerve (the lateral cutaneous nerve of the forearm).
The skin over the joint belongs anteriorlaterally to C6 dermatome and anteromedially to C5, C8, and T1 dermatomes. Posteriorly, the C6 dermatome laterally and the C8 dermatome medially are split down the middle by the C7 dermatome.
Blood Supply of Elbow Joint
The blood supply to the elbow joint is by the branches from the periarticular arterial anastomoses of the elbow.

Clinical Significance of Elbow Joint
Elbow joint is a frequently injured joint and site for many disorders
Dislocation of Elbow

Dislocation of elbow could occur in isolation or as part of more severe trauma which may cause fracture of the bones too.
Pulled Elbow
In children, when a distraction force is applied along the long axis of the forearm from a point distal to the elbow, the head of the radius can be pulled out of the annular ligament that holds it in place. This injury is called “pulled elbow” and occur in young children. The injury usually involves a parent or other adult figure lifting a child up vertically by a single hand.
Lateral epicondylitis
Lateral epicondylitis is also called tennis elbow and involves inflammation of the common extensor origin at the lateral epicondyle of the humerus. Repetitive extension movements at the wrist cause pain.
Medial epicondylitis
Medial epicondylitis or golfer’s elbow is an inflammation of the common flexor origin at the medial epicondyle of the humerus. Repetitive flexion movements at the wrist cause an overuse of pain at the site.
Cubital tunnel syndrome
Cubital tunnel syndrome is caused by compression of the nerve as it passes in a groove behind the medial epicondyle of the humerus or cubital tunnel. Paresthesias in the distribution of the ulnar nerve are the chief complaint.
Pronator syndrome
Compression neuropathy of the median nerve as it passes between the two heads of the pronator teres muscle. The syndrome can cause paresthesias in the distribution of the median nerve distal to the compression and may lead to weakness in the flexor pollicis longus, the flexor digitorum profundus laterally, and the pronator quadratus.
Olecranon bursitis
Olecranon bursitis or student’s elbow is an inflammation of the olecranon bursa at the proximal aspect of the posterior ulna. It can be caused by trauma, infection, prolonged pressure, or other conditions. The bursa is swollen and is often painful.